
Key Takeaways
|
1chap7_p_1This chapter, presented in two parts, provides a comprehensive overview of PPPs in the health sector. Part 1 explores the foundational aspects of health PPPs, beginning with an explanation of what PPPs are and the benefits they can bring to healthcare delivery. It examines the enabling conditions that contribute to successful implementation, compares traditional procurement methods with PPP approaches, and outlines the different types of health PPPs and their financing considerations. The section also emphasises the importance of effective stakeholder management in achieving project objectives.
2chap7_p_2Part 2 builds on this foundation by focusing on the practical dimensions of developing and managing health PPP projects. It provides technical guidance to the team designing and implementing the health PPP project. Specifically, it discusses how to build a pipeline of viable PPP projects, prepare and structure them for procurement, allocate risks appropriately and select suitable contractual models. The section concludes with guidance on the key contracts used by procuring entities and best practices for managing PPP contracts over their lifecycle.
Part 1: Understanding Health Public-Private Partnerships
Description and Rationale
3chap7_p_3PPPs are a globally recognised method of procurement. There is no single, internationally accepted definition of PPPs, but broadly speaking, a PPP can be defined as:
4chap7_p_4“A long-term contract between a private party and a procuring entity, for the provision of a public asset and/or service, in which the private party bears significant risk and management responsibility, and where remuneration is linked to performance.”
5chap7_p_5Procuring entities can include central government ministries, state departments, state agencies, state-owned entities and municipal entities. In a healthcare context, these entities typically include the Ministry of Health (MoH), health boards and hospital trusts (or equivalent entities), among others.
6chap7_p_6The duration of a PPP contract is typically between 10 and 30 years, allowing sufficient time for the asset to be affordable on an annual basis. However, the duration of a PPP contract can be shorter (e.g. for a service-only contract or digital health technologies) or longer (e.g. larger-scale projects where the private provider needs longer to recoup its investment).
7chap7_p_7Some key considerations related to PPPs include:
- chap7_ul_1
- chap7_li_9The functions for which the private party is responsible vary, but may include design, construction, renovation, financing, maintenance and operation.
- chap7_ul_2
- chap7_li_10PPP projects often involve the procurement of new assets; however, some PPP arrangements also involve the rehabilitation and/or maintenance of existing assets.
- chap7_ul_3
- chap7_li_11Risks are allocated to the party best able to bear them.
- chap7_ul_4
- chap7_li_12Each of the phases of the PPP project is generally addressed in one contract (e.g. a project agreement or concession agreement).
- chap7_ul_5
- chap7_li_13The private party typically operates through a special purpose vehicle (SPV), a separate, legally independent company that is created to carry out a specific project.
- chap7_ul_6
- chap7_li_14The payment mechanism in a PPP contract may include a tariff or user fee model, an availability-based model or a combination of these, with or without a subsidy. There will also typically be a performance management system with key performance indicators (KPIs) and a payment deduction mechanism.
- chap7_ul_7
- chap7_li_15PPPs can be applied across different sectors (including the health sector), but there might be some government limitations (e.g. some countries cannot have PPPs in the defence sector).
Rationale
8chap7_p_8PPPs can be an effective way of supporting UHC as they mobilise private sector financing and expertise, which can close the funding gap while bringing efficiencies into health systems. Governments should be clear on the issues they are seeking to solve by involving the private sector in healthcare delivery. This can take several forms or a combination thereof:
- chap7_ul_8
- chap7_li_16Closing the infrastructure gap. Through PPPs, governments can accelerate the delivery of infrastructure needed for a range of facilities such as clinics, hospitals and diagnostic centres without bearing the full upfront fiscal burden, while ensuring long-term performance and service quality through outcome-based partnership contracts.
- chap7_li_17Closing the medical equipment gap. PPPs enable access to medical technologies through various mechanisms, including leasing, build-operate-transfer (BOT) and managed equipment service (MES) models that improve clinical outcomes and operational efficiency. By aligning incentives between public health objectives and private sector innovation, PPPs help strengthen resilience, expand access to care and modernise health systems in a financially sustainable and scalable way.
- chap7_li_18Dealing with shortages in healthcare workers and specific skill sets. The shortage in healthcare workers (HCWs) and specialised skills is a significant global challenge. These issues are most profound in low and middle-income countries, particularly in Africa, which has 25% of the world’s disease burden but has only 3% of global HCWs. PPPs can work towards increasing the employment and utilisation of HCWs in Africa by providing additional employment opportunities, focusing on training and professional development, particularly in areas where there is a shortage of specialists, improving retention and optimising the utilisation of HCWs. Moreover, the private sector can leverage medical equipment, digital health technologies and artificial intelligence to enable healthcare delivery in resource-scarce environments.
Case Study: Applicability of PPP in the Improvement of Clinical Services and Renovation of Existing Facilities9chap7_p_9The Ministry of Public Health had received a public hospital from a donor but was unable to operate the hospital to acceptable clinical standards. The need to improve clinical services, as well as renovate the existing facilities and develop a new pharmaceuticals facility, led the Ministry to explore the possibility of harnessing private sector investment and managerial skills for the hospital. The Ministry outlined its requirements for the core clinical services to be provided to patients, including maternity health services, neonatology services, paediatric health services, oncology, medical, surgical and radiotherapy services, as well as diagnostic services. A key consideration was the patient mix, ensuring that not only private patients but also a percentage of low-income patients could access the enhanced facilities at no cost. |
- chap7_ul_9
- chap7_li_19Improving operational efficiency and realising cost savings. PPPs can improve operational efficiency and realise cost savings in healthcare systems by introducing private sector innovation, management expertise and performance-driven accountability into the delivery of healthcare services. Through well-structured PPP contracts, the public sector can shift from input-based spending to outcome-based models (value-based healthcare) that reward efficiency, quality and patient satisfaction. The private sector’s ability to optimise workflows, deploy digital health solutions and implement preventive maintenance systems can reduce inefficiencies in hospital operations. Economies of scale can be achieved through integrated procurement, supply chain management and shared service models. The public partner must be able to meet its payment obligations and monitor outcomes and KPIs.
Enabling Conditions
10chap7_p_10To incentivise investments in healthcare PPP projects, countries need a transparent, stable and predictable investment ecosystem that allows for transparent and efficient contracting processes and contract enforcement. This needs to be underpinned by sound health policies and embedded into institutions that enable the private sector, both domestic and international, to operate efficiently, profitably and with maximum development impact. Therefore, promoting and protecting health-related investments requires special emphasis from governments to ensure that appropriate regulatory and policy frameworks are in place.
11chap7_p_11Potential investors will assess the domestic legal and regulatory environment in the relevant country before deciding to participate in any healthcare PPP project. Each country will have their own legal and regulatory considerations and risks, which will naturally impact the nature and extent of any investment that may be provided for a specific healthcare PPP project. Any such assessment will need to be carried out by potential investors on a case-by-case basis, and each investor will have their own particular requirements that must be satisfied before any investment is contemplated.
12chap7_p_12A list of the common issues or risks that need to be considered by investors as part of their country due diligence before investing in health PPP projects includes:
- chap7_ul_10
- chap7_li_20The rule of law is a fundamental pillar and indicator of a country’s readiness for investment. Linking to a variety of risk categories, including a country’s legal and regulatory environment, control of crime and corruption, and disputes, the rule of law underpins the legal certainty in and of a jurisdiction.
- chap7_li_21The legal and regulatory environment allows investments (foreign direct investment limits, bankruptcy and insolvency laws and investment and assurance laws).
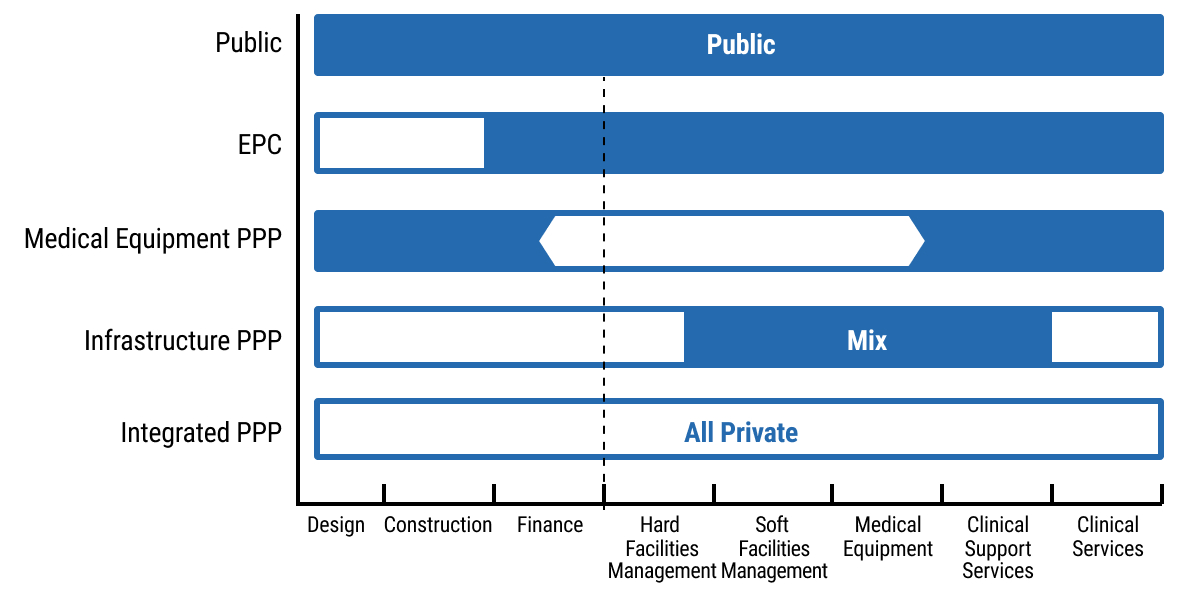
- chap7_li_22The availability of international arbitration as a dispute resolution mechanism.
13chap7_p_13There should be a solid legal framework which clearly applies to health PPP projects. A critical part of this framework is having a robust PPP law. The key requirements for an effective PPP law include:
- chap7_ul_11
- chap7_li_23Harmonisation of the institutional framework for the implementation of PPP projects, which would apply to health projects.
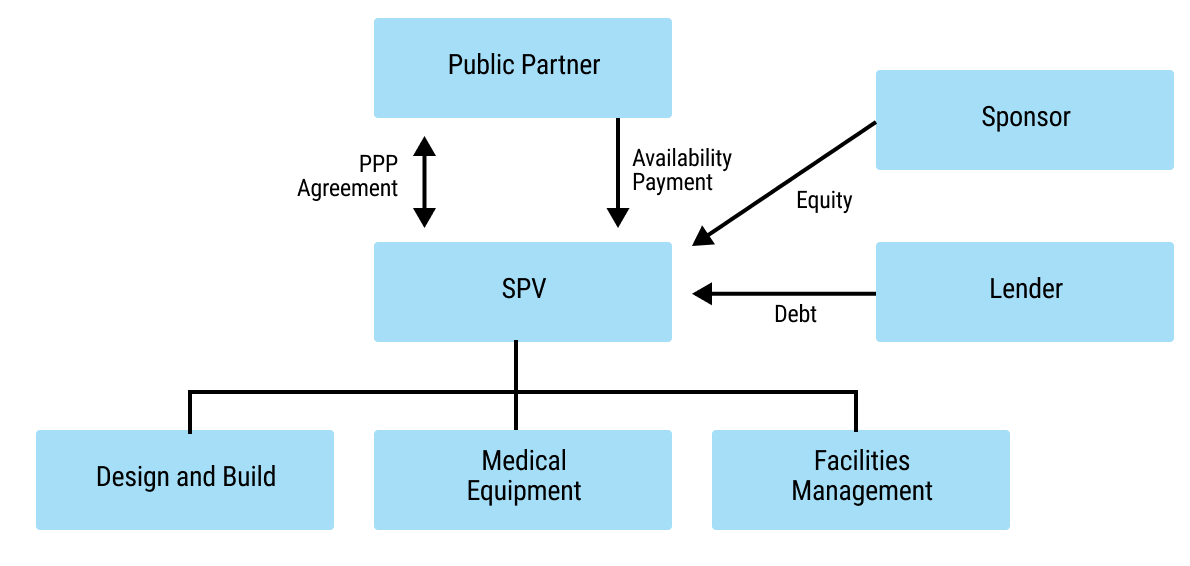
- chap7_li_24Enabling the participation of the private sector in the development and implementation of PPP projects, including through the incentivisation of public/private collaboration.
- chap7_li_25Provision for clear procurement procedures, including guidelines on competitive procedure and the unsolicited procedure.
- chap7_li_26Identification of the types of state support which may be available for health PPP projects on a case-by-case basis, such as sovereign guarantees and undertakings, viability gap financing, subsidies, tax exemptions and/or benefits (See also Chapter 8: Credit Enhancement).
Challenges
14chap7_p_14In Table 7.1 below, we have identified a selection of typical challenges that can adversely affect the implementation of health PPPs, along with suggested solutions for each challenge.
|
15chap7_p_15Typical Challenge |
16chap7_p_16Solution |
|
17chap7_p_17Inadequate legal framework, policies and enforcement |
18chap7_p_18There should be a solid legal, policy and regulatory framework which clearly applies to health PPP projects. This should include laws relating to PPP, procurement, investment and private sector participation in healthcare. 19chap7_p_19A robust institutional framework is usually best enforced through a central PPP unit, typically housed within the Ministry of Finance (MoF). |
|
20chap7_p_20Lack of prioritisation within government ministries or interference from government ministers which can lead to delays. 21chap7_p_21 |
22chap7_p_22There should be political will to support health PPPs and ongoing political stability. Long-term health PPP projects need appropriate long-term support. To avoid interference, proper governance and approvals procedures should be introduced and consistently applied. |
|
23chap7_p_23A weak payment mechanism for remunerating the private partner (e.g. public and/or mandatory private health insurance or inadequate remuneration levels). |
24chap7_p_24This does not enable payments to be output-based. While it does not prevent PPP schemes from proceeding, the payment mechanism will be based on cost reimbursement and a margin. |
|
25chap7_p_25Lack of capacity and capability among government officials. 26chap7_p_26 |
27chap7_p_27A programme of health PPP capacity building should be introduced to ensure that there are trained and experienced public sector personnel, focused on delivery. |
|
28chap7_p_28Lack of interest from tenderers, possibly due to a lack of knowledge about the jurisdiction and publicity about the health PPP programmes/projects. |
29chap7_p_29The procuring entity should publish a visible and credible pipeline of health PPP projects. It is recommended that the procuring entity carry out preliminary market engagement with the private sector market and understand what might be the competing projects to their health PPP programme. |
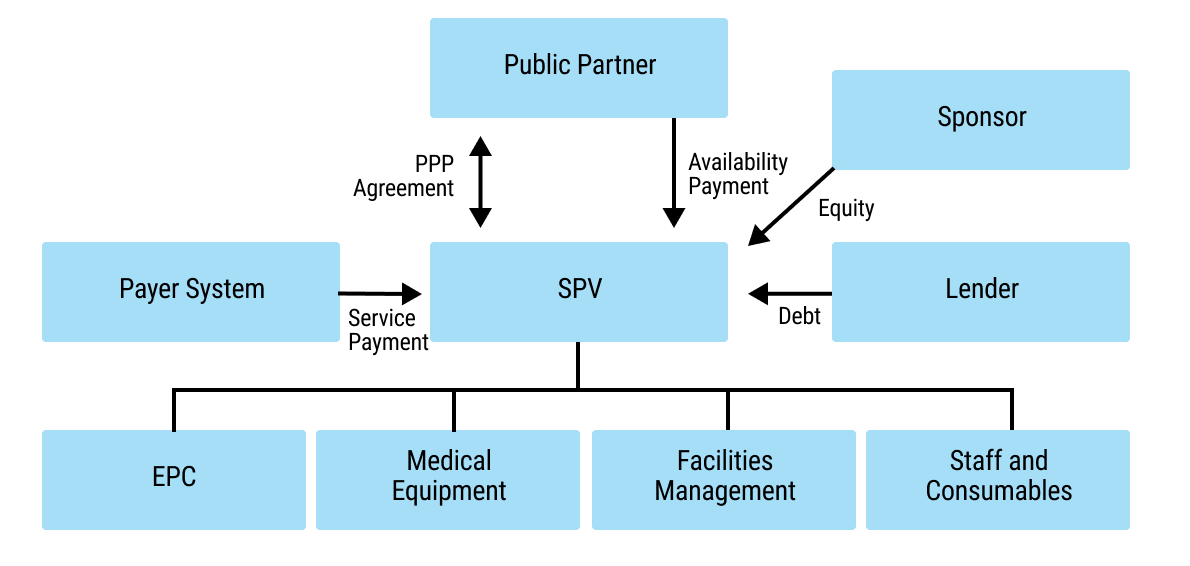
|
30chap7_p_30Poor contract packaging occurs when PPP contracts are too small, too diverse or too risky. 31chap7_p_31 |
32chap7_p_32The procuring entity should undertake comprehensive feasibility studies and business cases as part of preparing the PPP project. Bundling projects together or separating them into parts may be advisable to match the scope that the market is ready to undertake. |
|
33chap7_p_33Inappropriate or unrealistic risk transfer, for example, occurs when all risks are fully allocated to the private partner. |
34chap7_p_34The procuring entity should undertake a full risk assessment of the proposed PPP project. |
|
35chap7_p_35Failure to comply with and/or apply health PPP contractual provisions, which can result in delays, disputes, fraud and corruption. |
36chap7_p_36The procuring entity should undertake robust contract administration. |
|
37chap7_p_37Failure to establish strong stakeholder arrangements. |
38chap7_p_38It is essential to engage all necessary stakeholders and manage their expectations, and to spend time planning and managing both the development and implementation of the health PPP. |
|
39chap7_p_39Relegation of sustainability considerations |
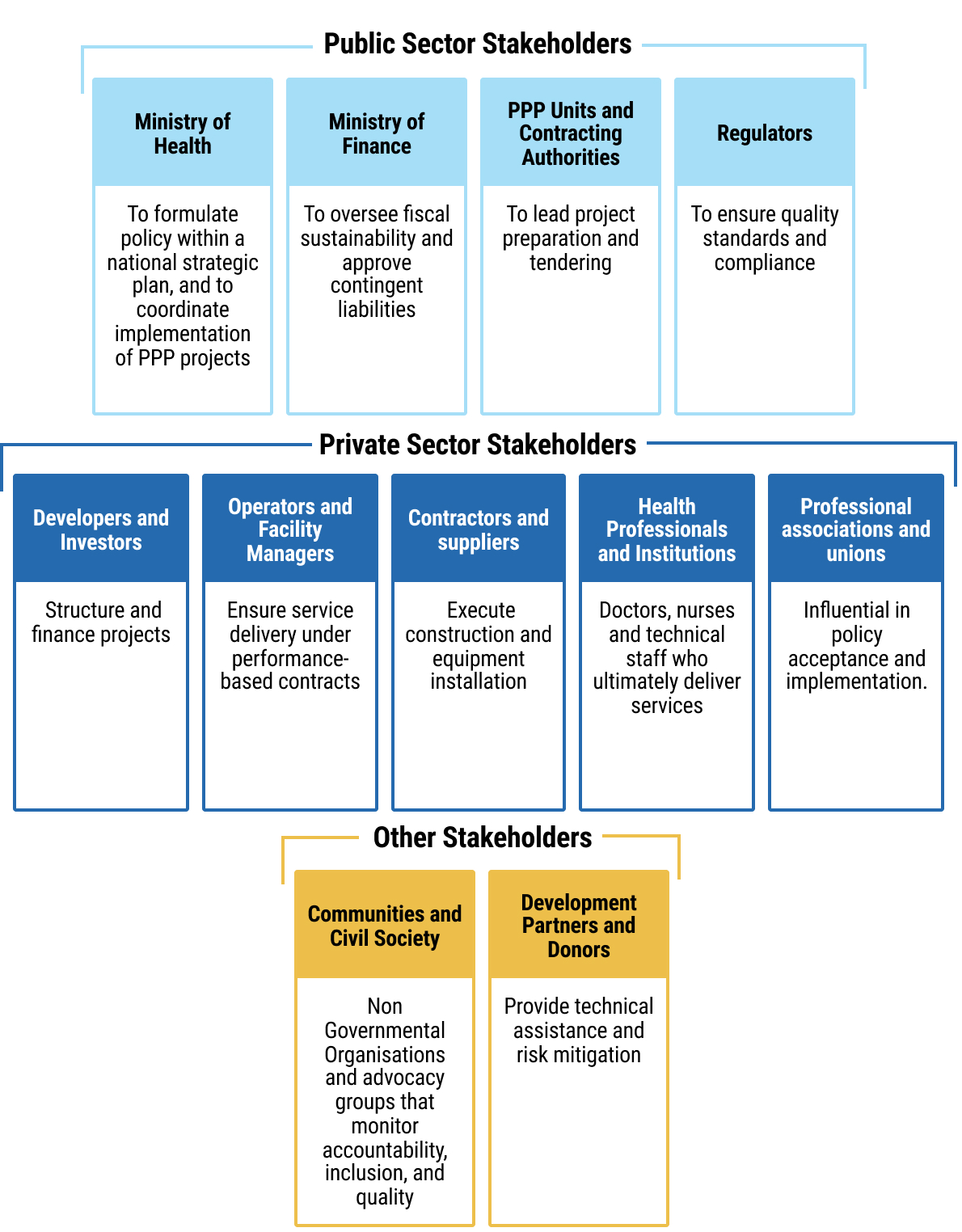
40chap7_p_40Environmental, social and governance (ESG) principles align closely with public health objectives - reducing waste, improving working conditions and ensuring equitable access to care. ESG considerations should be built into health PPP procurement and operation (e.g. sustainable hospital design or climate-resilient infrastructure). |
Types of Health PPPs
41chap7_p_41Health projects can be procured in several ways, ranging from full public delivery to arrangements where private partners are responsible for ongoing service provision. This chapter focuses on PPPs where the private partner contributes private finance and delivers the project. The chapter does not include engineering, procurement and construction (EPC) projects where the private provider does not provide an ongoing service after the completion of the construction phase.
42chap7_p_42Figure 7.1 illustrates the continuum of procurement from fully public to PPP models. This section elaborates on how PPP models, shown at the latter end of this spectrum, are used to deliver specific activities in the health sector.
 chap7_img_0
chap7_img_0
43chap7_p_43Various types of PPPs are described briefly below.
Infrastructure PPPs
44chap7_p_44In infrastructure PPPs, the private partner undertakes the planning, design, construction, equipping, financing, facilities management and non-clinical services while the public partner is responsible for the clinical services. This method has been widely adopted in the U.K., Canada, Australia, Europe and recently in Saudi Arabia.
45chap7_p_45The diagram below presents a simple organisation chart showing how the parties in an infrastructure PPP are interrelated. The private partner is shown as an SPV, which enters into the PPP agreement with the procuring entity (shown as the Public Partner) and receives payment from the public partner in the form of an availability payment (a payment made once the asset is available for use per the contract). The funding comes primarily from the sponsor (or investor) as equity and from the lender as debt. The SPV then enters into subcontract arrangements for the design and build of the facility, for providing and installing medical equipment, and for undertaking facilities management.
 chap7_img_1
chap7_img_1
46chap7_p_46Infrastructure PPPs typically have long tenors of 20-30 years, and require financing with favourable terms to keep the cost of capital affordable.
47chap7_p_47The private partner typically receives an availability payment for making the asset available and a service payment for providing the non-clinical services.
48chap7_p_48The hospital’s capacity is planned to meet the public sector’s requirements, often leaving limited scope for optimising the design and operations. This model is attractive to funders and investors as it carries no demand risk. The private partner’s key risks are the completion of the development works on time and meeting the availability criteria, as well as ensuring the facility meets its key performance requirements.
49chap7_p_49The PPP can additionally help incentivise efficiencies within the private partner. For example, the private partner could be responsible for energy and water consumption costs at a set tariff. This shares the risk between the public and private partners, with the private partner designing and building energy-efficient buildings and the public provider incurring the risk if the tariff rate increases.
Case Study: Private Sector Innovation Through a New Health PPP Model in the U.K.50chap7_p_50The New Velindre Cancer Centre (nVCC) is one of three Welsh Government pilot projects and the first hospital to use the new Mutual Investment Model (MIM). This model includes a 15% public sector stake in the SPV and a significant community benefits package mandated through procurement. Key innovations include:
|
Medical Equipment PPPs
51chap7_p_51Similar to infrastructure PPPs, in the medical equipment PPP model, the private partner undertakes the planning, design, equipping, and, if needed, any construction or retrofitting. In addition, the private partner finances the project and undertakes the maintenance and any facilities management services associated with the medical equipment and its surroundings.
52chap7_p_52There are two options for operating the medical equipment itself:
- chap7_ul_13
- chap7_li_30By the public partner, in which case the model is akin to an infrastructure PPP.
- chap7_li_31By the private partner, where the public partner would be required to agree on the diagnostic service volumes and agree to a set of tariffs.
53chap7_p_53
54chap7_p_54This PPP type typically has shorter tenures of 7-12 years, which is compatible with the life cycle of the equipment.
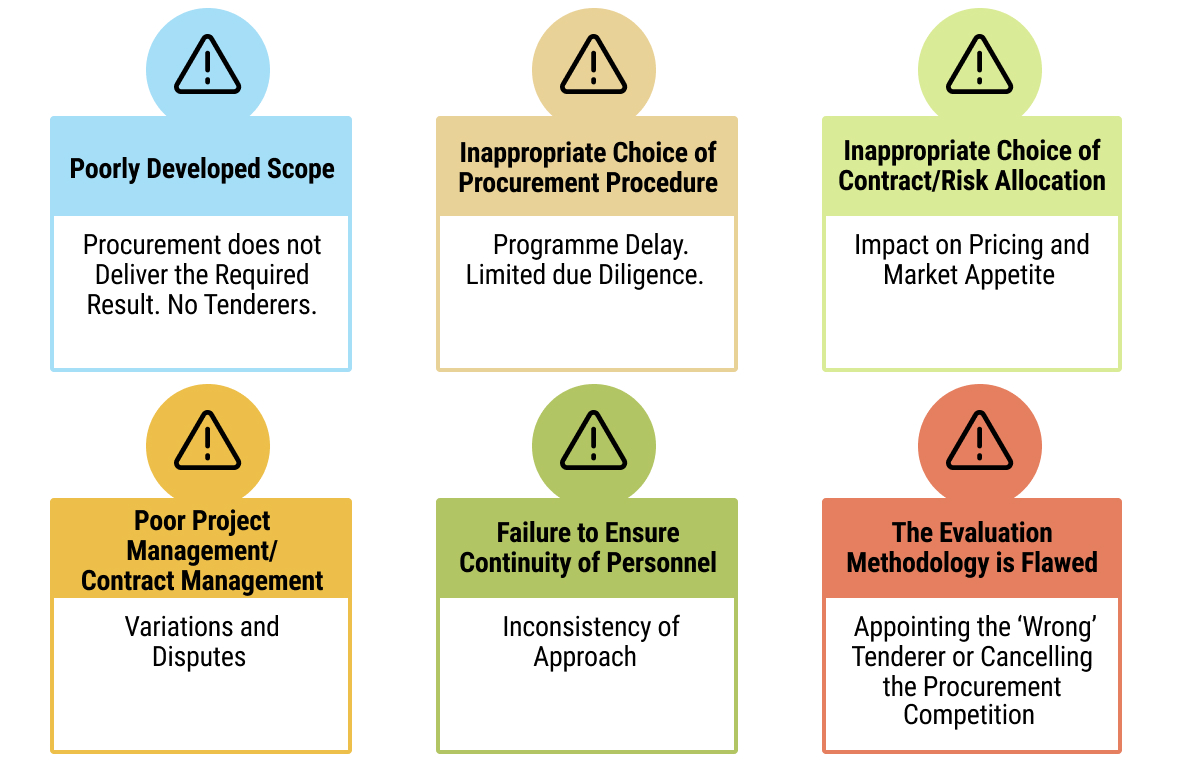
Case Study: Managed Equipment Services (MES) in Kenya55chap7_p_55The Kenyan government entered into contracts with several original equipment manufacturers (OEMs) to enhance access to and equity in healthcare. Under the MES arrangement, OEMs were responsible for supplying, installing, maintaining and replacing medical equipment, as well as providing user training across hospitals nationwide. 56chap7_p_56The MES programme was successfully implemented, significantly upgrading specialised health infrastructure and expanding access to critical healthcare services nationwide. Previously unavailable services, such as dialysis, critical care, surgical theatres, sterilisation and advanced imaging, were introduced or expanded in multiple hospitals. 57chap7_p_57The programme ensured reliable equipment installation and maintenance, enhanced the capacity of healthcare workers (HCWs) through training and fostered a more enabling work environment. Key lessons learned included the importance of: (i) defining detailed equipment specifications, (ii) ensuring comprehensive stakeholder engagement, and (iii) allocating sufficient time for assessment, procurement, and implementation. |
Digital health PPPs
58chap7_p_58Digital health PPPs support the transformation of healthcare businesses and sector-wide processes and operations by adopting digital technology, creating new opportunities and driving change. PPPs in digital health typically require combining the agility of the private sector with public sector access to patients and medical records. They tend to have even shorter tenors, given the short lifespan of these technologies. These partnerships rely on speedy implementations of ready solutions or those at the beta test stage.
59chap7_p_59
Case Study: Digital Health - Estonia, Electronic Health Record60chap7_p_60Estonia’s journey towards digital healthcare has involved collaboration between the government and various technology providers to develop, implement and manage its national electronic health record (EHR) and e-Health systems. While the specific details of the agreements and partnerships that facilitated the rollout of Estonia’s EHR system may vary and involve multiple contracts and collaborations, the overarching strategy aligns with the PPP model. This model leverages both public oversight and governance, as well as private sector innovation and efficiency, to achieve public health goals. Its digital health ecosystem, known for its e-Health Record system, integrates data from various healthcare providers, providing patients and doctors with online access to medical histories, prescription information and test results. 61chap7_p_61This initiative has significantly enhanced the efficiency of healthcare delivery, improved patient safety and strengthened data security. According to the Estonian e-Health Foundation, the system has led to a 30% reduction in duplicate testing, saving time and resources. |
Case Study: Artificial Intelligence - United Kingdom, Google and the National Health Service62chap7_p_62The collaboration between Google’s DeepMind and the U.K.’s National Health Service on improving eye disease detection through AI technology exemplifies successful PPPs in healthcare. This project utilised AI to analyse eye scans for conditions such as diabetic retinopathy and age-related macular degeneration, which specialists traditionally diagnose. By leveraging DeepMind’s artificial intelligence to interpret optical coherence tomography (OCT) scans, the partnership aimed to enhance diagnostic speed and accuracy. Trained on a vast dataset of de-identified OCT scans from Moorfields Eye Hospital, the AI system matched the accuracy of leading experts in identifying eye diseases. This collaboration enhanced diagnostic efficiency, alleviated specialists’ workload through automation, and demonstrated the potential for scaling AI solutions across the healthcare system. |
Training and education PPPs
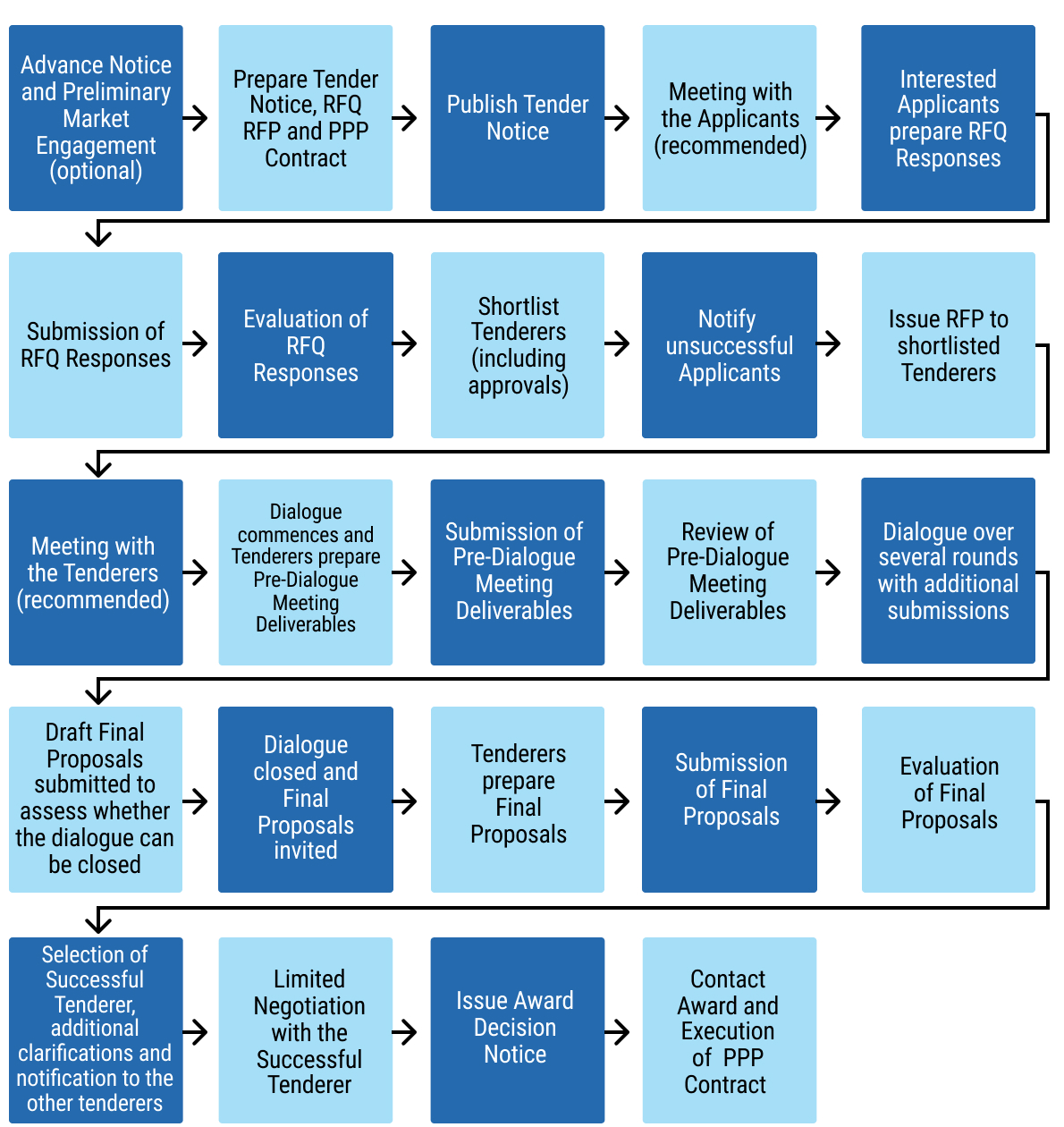
63chap7_p_63Where the construction of a training institution is required, a PPP could be used, similar to infrastructure PPPs. This could be extended to a model where the private partner provides the facilities and pedagogical services (I.e. gives pre-service training to HCWs).
Private Wings in Public Facilities
64chap7_p_64Under the private wings in the public facilities model, a public hospital enters into an arrangement with a private partner to establish a private patients’ wing on its premises. In that case, the private partner attracts private paying patients and admits them to that wing, providing all the hotel services (e.g. catering) while utilising the diagnostic and treatment services offered at the hospital to public patients. This arrangement typically takes the form of a lease or sublease of the private patient wing, with admission rights granted and a service level agreement (SLA) in place for the services provided by the public hospital. The SLA specifies matters such as response times, prices, risk and liability.
Case Study: Expansion of Commercial Activities at a Public Hospital65chap7_p_65A public hospital in the U.K. had already expanded its commercial activities with the objective of cross-subsidising the costs of public healthcare. As part of its commercial strategy, the public hospital assessed the potential to further increase the profitability of its private patient income, generating additional funds to reinvest in public hospital services. The benefits of using the Private Patient Admissions model included:
66chap7_p_66 |
Integrated PPPs
67chap7_p_67The Integrated PPP model involves comprehensive outsourcing, whereby planning, design, construction, equipping, staffing, financing, operations and management are outsourced on a long-term contract basis to a private partner. This PPP type introduces significant efficiencies into the operations as the contracting is based on a set of clinical activities, not based on capacity parameters - such as bed count - (as is the case with infrastructure PPPs).
68chap7_p_68The diagram below provides a simple organisation chart showing how the parties in an integrated PPP are interrelated. The private partner is shown as an SPV, which enters into the PPP agreement with the public partner and receives payment from the public partner in the form of an availability payment. In addition, the SPV receives payment for clinical services provided to patients, typically from the payer system (e.g. the public partner or national health insurance scheme). The funding it receives comes primarily from the investor (or sponsor) as equity and from the lender as debt. The SPV then enters into subcontract arrangements for the design and build of the facility, for providing and installing medical equipment and for undertaking facilities management. Importantly, the SPV is responsible for all the inputs required to deliver clinical services to patients, including hiring staff and procuring all necessary consumables.
 chap7_img_2
chap7_img_2
69chap7_p_69The payment mechanism can be calculated based on the catchment population (I.e. a capitation system) or using a fee-for-service model (e.g. using diagnostic-related groups), or a combination of both.
Case Study: La Ribera Hospital, Valencia, Spain70chap7_p_70This PPP combined the development and operation of a 300-bed hospital with four integrated healthcare centres and 46 public primary care centres, covering a catchment population of 250,000 people in the Alzira region. The project was structured as a 15-year concession (5-year extension option) with payment on a capitation basis. Payment covered the entire care continuum for patients, which incentivised the provider to encourage the population to undergo screening, preventative and awareness programmes. 71chap7_p_71This resulted in improved patient satisfaction and increased efficiency, with shorter waiting lists, lower lengths of stay and higher utilisation of surgical theatres. |
Case Study: Managing Capacity Constraints in a Health Sector PPP72chap7_p_72A major healthcare PPP in a lower-income country illustrated that, while such arrangements can improve healthcare infrastructure and service delivery, strong government capacity and effective contract management are critical for success. The project, which replaced a national referral hospital and introduced new clinical services, initially achieved higher-quality care and efficiency. 73chap7_p_73However, costs escalated dramatically due to weak oversight, unclear risk allocation and inadequate financial controls, consuming an unsustainable share of the national health budget. The main lesson learned is that PPPs in social sectors such as health require robust institutional capacity, transparent monitoring and flexibility to adjust terms over time to prevent fiscal strain and ensure long-term sustainability. |
Management Contracts
74chap7_p_74The management contracts PPP model is used in countries where there is insufficient capacity in the public system and/or resources to operate its hospitals. In such cases, a facility would be built, and then a private operator would be brought in to commission and manage it.
Purchasing Services
75chap7_p_75Under a purchasing services model, the public health system purchases specific procedures from the private sector, such as dialysis, diagnostics, angiograms and certain surgeries.
Financing Considerations
76chap7_p_76PPP projects are typically financed using a range of financial instruments, each bearing a level of risk and attracting a certain cost of capital. By allocating different levels of risk across the capital structure, it is possible to have a more acceptable weighted average cost of capital (WACC). Typical instruments found across the capital structure are listed below (in decreasing order of risk):
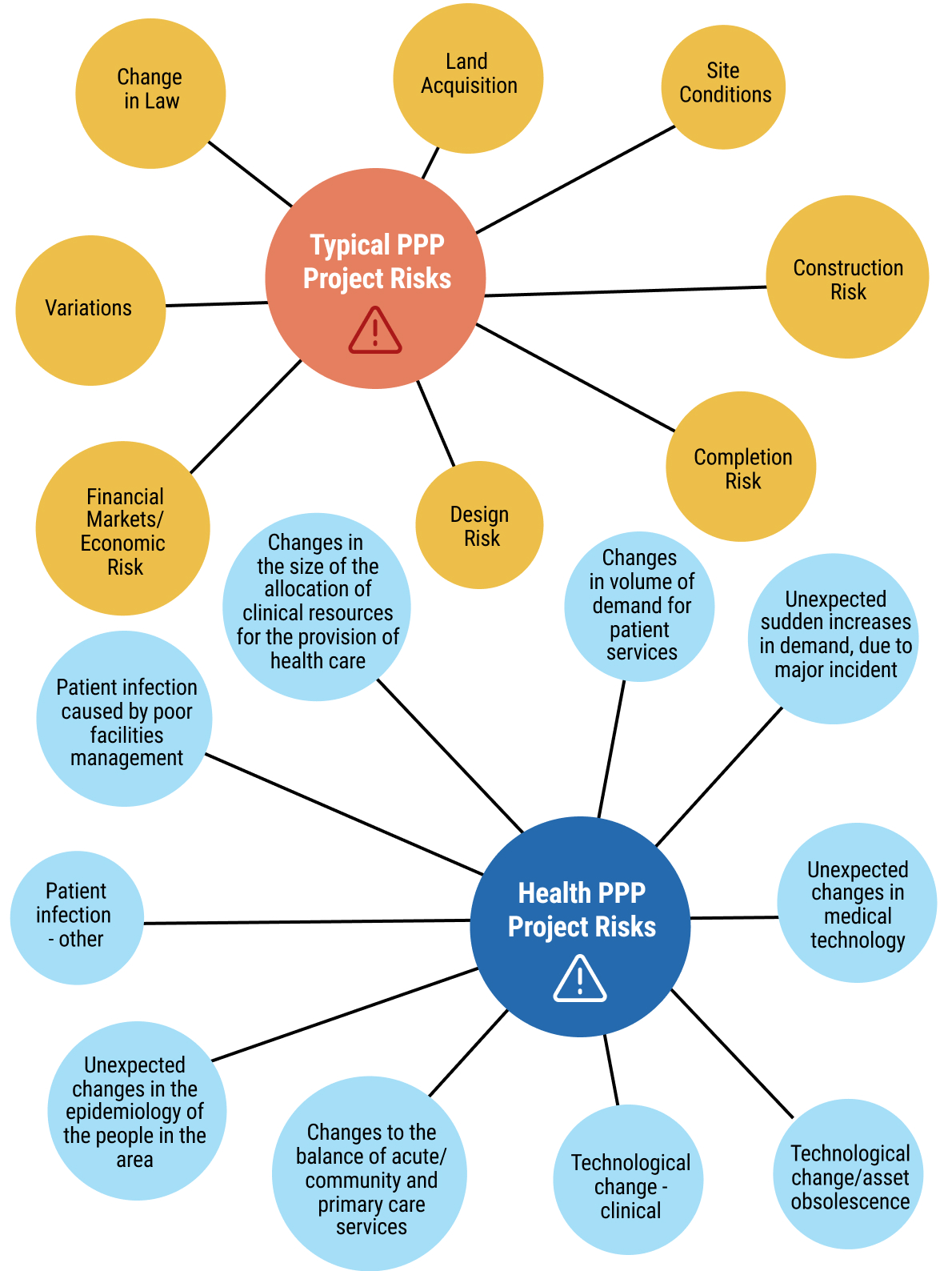
- chap7_ul_15
- chap7_li_37Equity. This is the capital invested by the private partner to own the project (or part thereof), taking on the highest risk but also receiving the highest potential return. Unlike investors in debt instruments, equity investors are owners with a stake in the project’s success and are liable for any initial losses.
- chap7_li_38Quasi-equity. This type of financing falls between a traditional loan and an equity investment. It behaves somewhat like shares - because the investor can earn a higher return and, in some cases, the loan can later be converted into an ownership stake - but it does not give the investor control or equity from the outset. It is sometimes referred to as mezzanine or subordinated debt. Because it carries more risk than a standard loan, the investor receives a higher, fixed return (similar to a guaranteed dividend). This kind of capital can help make a health PPP viable by filling the gap between regular bank loans and full equity investment.
- chap7_li_39Senior debt. This refers to the debt that takes priority over other types of financing, in the event of a default or liquidation. It is typically the first to be repaid before others in the capital structure. In PPPs, senior debt is usually provided by banks or other financial institutions and is secured against the project’s assets and proceeds, ensuring a lower risk for the lenders. Senior debt can also be arranged as a bond issue. See also Chapter 5: Sustainable Finance Instruments for a description of bonds and loans. Given its priority, senior debt often comes with lower interest rates compared to junior debt. A key component in the financing structure of PPP projects is providing funding for the initial capital investment required for infrastructure projects.
77chap7_p_77An essential aspect of making healthcare projects more affordable and sustainable is to introduce efficiencies in the design and delivery of the infrastructure and remove unnecessary costs in service delivery. However, in the context of a PPP, it is also essential to lower the WACC of the project by:
- chap7_ul_16
- chap7_li_40Maximising the amount of senior debt.
- chap7_li_41Lowering the cost of senior debt.
- chap7_li_42Lowering the cost of equity by introducing quasi-equity instruments to the extent permissible under the PPP law or the PPP agreement.
- chap7_li_43Utilising viability gap funding in one or more of the forms listed below, and blending them with equity and, as required, quasi-equity and senior debt. This serves as a form of credit enhancement (see Chapter 8: Credit Enhancement for more details). This mechanism is referred to as blended finance and could leverage:
- chap7_li_44Grant funding that could be provided by the public sector or by donor partners.
- chap7_li_45Concessional loans, supplied by development finance institutions (DFIs) or multilateral development banks (MDBs).
- chap7_li_46Debt-for-health swaps (see Chapter 6: Debt-for-Health Swaps) could generate financial flows over time to enhance the PPP financing structure.
- chap7_ul_17
78chap7_p_78To maintain the oversight and governance structure that can be required to manage blended finance resources, special trust funds may be set up for disbursing the funds and overseeing the achievement of the applicable health programme and/or KPIs.
79chap7_p_79Channelling blended finance into PPP projects comes with the benefit of financial sustainability. These additional resources will lower the WACC, making the project more affordable to the government and/or to users.
80chap7_p_80Beyond the mobilisation of financing instruments, there are key financial considerations that are inherent to the PPP project, some of which have already been mentioned in the section above on Enabling Conditions:
- chap7_ul_18
- chap7_li_47Demand risk. The extent to which demand risk is transferred to the private partner in the first place. If demand risk is transferred, whether this is accompanied by a minimum patient volume guarantee, such that utilisation rates are predictable and sufficient to ensure revenue stability for the private partner.
- chap7_li_48Payment mechanism. Clarity and reliability of how the private party is paid (e.g. availability payments, service fees, user tariffs or combination thereof).
- chap7_li_49Government support. Extent and enforceability of guarantees, subsidies or minimum revenue undertakings to enhance financial confidence.
- chap7_li_50Creditworthiness of offtaker. The financial health and payment history of the government or public entity making payments.
- chap7_li_51Tariff or fee setting. Establishing a tariff in the first place, and if so, the ability to adjust tariffs or payments in line with inflation, cost changes or performance targets.
- chap7_li_52Project preparation. Quality of feasibility studies, demand forecasts and risk allocation frameworks underpinning the project.
- chap7_li_53Regulatory environment. Clarity, predictability and stability of healthcare and PPP regulations affecting licensing, pricing and service delivery.
- chap7_li_54Political and policy stability. Government commitment to the PPP structure and avoidance of arbitrary policy changes.
- chap7_li_55Risk allocation. Appropriate distribution of construction, demand, operational and regulatory risks between public and private parties.
- chap7_li_56Land and site issues. Secure access to the project site, clear title and timely availability of utilities and supporting infrastructure.
- chap7_li_57Approvals and licensing. Streamlined processes for health facility accreditation, environmental and operational approvals.
- chap7_li_58Performance standards. Precise service level requirements and measurable KPIs linked to payments.
- chap7_li_59Termination regime. Fair compensation framework in the event of early termination due to government or private default.
- chap7_li_60Step-in rights. The right of lenders to step in and cure defaults before termination to protect their interests.
- chap7_li_61Currency and forex risk. Mechanisms to mitigate foreign exchange volatility where financing is in hard currency but revenues are local.
- chap7_li_62Dispute resolution. Efficient, neutral and enforceable mechanisms (e.g. arbitration) for resolving contractual disputes.
- chap7_li_63ESG and social impact. Compliance with environmental, social and governance standards and alignment with public health goals.
- chap7_li_64Capacity of public counterparty. Institutional ability to manage and monitor complex PPP contracts over the project lifecycle.
- chap7_li_65Bankable documentation. Well-drafted concession, project and finance agreements that align with lender requirements.
Stakeholder Management
81chap7_p_81Health PPPs bring together diverse actors drawn from government agencies, financiers, developers, operators, healthcare professionals and communities. The success or failure of these partnerships often hinges on how stakeholders are identified, engaged and managed throughout the PPP lifecycle. This section explores the critical role of stakeholders in health PPPs, emphasising stakeholder management, cross-governmental collaboration and best practices that drive successful project outcomes.
82chap7_p_82The first step involves mapping the stakeholder landscape in health PPPs to identify who matters most, their level of influence and potential risks associated with ignoring their interests. The typical players who are engaged in health PPPs are:
- chap7_ul_19
- chap7_li_66Public Sector Stakeholders such as the MoH, MoF, PPP units and procuring entities (also known as contracting authorities) and regulators.
- chap7_li_67Private Sector Stakeholders such as developers and investors, operators and facility managers, contractors and suppliers, health professionals and institutions, professional associations and unions.
- chap7_li_68Other stakeholders include development partners, donors, communities and civil society more broadly.
 chap7_img_3
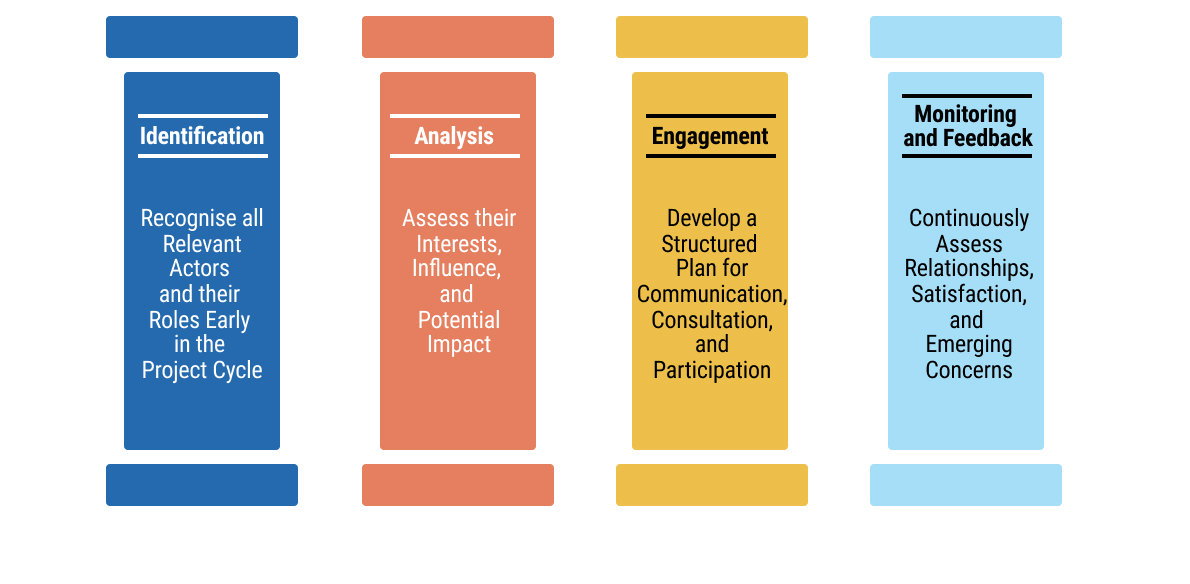
chap7_img_383chap7_p_83The second step is stakeholder management, a strategic process that ensures alignment, communication and collaboration among actors with differing interests. The four pillars of stakeholder management consist of identification, analysis, engagement and monitoring/feedback:
 chap7_img_4
chap7_img_4
84chap7_p_84Common challenges in stakeholder engagement include:
- chap7_ul_20
- chap7_li_69Asymmetric information between technical agencies and communities.
- chap7_li_70Competing priorities among ministries, e.g. the MoF and the MoH.
- chap7_li_71Limited stakeholder capacity to understand complex PPP structures.
- chap7_li_72Resistance from health workers when not adequately consulted.
85chap7_p_85
Case Study: Underestimating the Influence of Professional Stakeholders86chap7_p_86One health-sector PPP demonstrated the significant risks that can arise when stakeholder engagement is insufficient during project preparation. The initiative, aimed at enhancing service delivery through private sector participation in a major public hospital, encountered strong resistance from health professionals. Their objections stemmed from limited consultation and a lack of transparency around the proposed involvement of a private partner in managing selected clinical services within a public facility. 87chap7_p_87Health workers expressed concern that the PPP project could undermine job security, professional autonomy and the quality of patient care. The absence of structured dialogue and communication channels led to mistrust, culminating in legal action against the government. The ensuing dispute generated reputational and political risk, discouraged potential bidders, and ultimately, the project was considered for restructuring and retendering. 88chap7_p_88This case study highlights a recurring challenge in health PPPs - the underestimation of professional stakeholder influence. Health workers, as frontline service providers, hold both technical expertise and moral authority that can shape public and policy perception. Failing to meaningfully engage them early in the project cycle can therefore jeopardise project legitimacy and investor confidence. This example highlights the importance of governments establishing formal stakeholder engagement frameworks, including structured consultations with professional associations, transparent communication of project objectives and mechanisms for addressing concerns related to employment and service quality. Proactive engagement not only mitigates resistance but also builds ownership, enabling smoother implementation and greater sustainability of health PPP projects. |
Case Study: Weak Stakeholder Coordination Undermining Health PPP Implementation89chap7_p_89One health-sector PPP demonstrated how insufficient stakeholder management can compromise the effectiveness of otherwise well-structured initiatives. The partnership, intended to expand reproductive and child health services through collaboration with non-state providers, faced significant implementation challenges arising from unclear roles, weak communication and limited involvement of frontline health personnel. Divergent expectations among stakeholders, coupled with the absence of structured dialogue, contributed to mistrust, slow decision-making and uneven service delivery. 90chap7_p_90The study further revealed that local government authorities lacked the capacity and governance systems necessary to coordinate multiple actors within the partnership. Power imbalances between public and private partners, combined with inadequate monitoring mechanisms, meant that accountability was weak and collaboration often depended on personal rather than institutional relationships. This experience highlights a central lesson for health PPPs: without deliberate, well-resourced stakeholder engagement and clear governance arrangements, even promising partnerships struggle to achieve their intended impact. |
Case Study: Vietnam - The Critical Importance of Stakeholder Engagement in Health Sector Reform91chap7_p_91Vietnam’s experience with PPPs demonstrates the critical importance of stakeholder engagement in health sector reform. As the government explored converting public hospitals into PPP-operated facilities, the World Bank’s report Public-Private Partnerships for Health in Vietnam: Issues and Options found that resistance quickly emerged - not because the PPP model was technically weak, but because many stakeholders felt uninformed and uncertain. Clinicians, hospital managers and frontline workers worried about losing professional autonomy, facing new performance pressures or seeing patient care compromised by commercial priorities. 92chap7_p_92Public perception posed an equally significant barrier. Communities viewed public hospitals as social assets that should remain accessible to all. Without clear communication, many feared PPPs would lead to higher user fees or reduced access for poorer households. Political actors, sensing public unease, grew cautious about championing PPP reforms. This lack of coordinated communication created an environment where rumours and misconceptions spread faster than official information, weakening confidence in the reform process. 93chap7_p_93The Vietnam case shows that the success of PPPs depends as much on managing people, expectations and trust as it does on financial or technical design. Transparent communication, early consultation with clinicians and proactive public outreach are crucial in reducing fear and building legitimacy. The core lesson is clear: without deliberate stakeholder engagement, even well-designed PPP initiatives risk delay, opposition or failure - while effective engagement can transform reforms into shared, socially supported solutions. |
94chap7_p_94Cross-governmental collaboration is essential to deliver a PPP and ensure coherence in policy, financing and service delivery. Often, MoHs lead project design without adequate coordination with the MoF and Planning. This leads to delays, unclear mandates and inconsistent expectations. Some mechanisms could help address those coordination challenges:
- chap7_ul_21
- chap7_li_73Establishing inter-ministerial committees to align decision-making among key ministries and scoping responsibilities across agencies
- chap7_li_74Establishing a PPP committee to provide a unified project governance structure
- chap7_li_75Joint planning and budgeting to harmonise resource allocation between the MoFs and MoHs
95chap7_p_95These mechanisms could benefit from consistently applying some of the following principles:
96chap7_p_961. Engage early and continuously. Involve stakeholders from project identification through to operations. Early engagement reduces resistance and improves design relevance.
97chap7_p_972. Ensure transparency and communication. Public disclosure of project information enhances trust. Use communication plans that are proactive and multi-channel, e.g community meetings, social media and local radio.
98chap7_p_983. Institutionalise participation. Establish stakeholder advisory forums or oversight committees that meet regularly to discuss project progress and address grievances.
99chap7_p_994. Build capacity. Train both public and private actors on PPP processes, risk sharing and performance monitoring.
Part 2: The Preparation, Procurement and Delivery of Health PPP Projects
100chap7_p_100Health PPP projects generally involve high-value, complex procurements. Careful preparation and management, both before, during and after the procurement competitions, will be required to ensure the successful delivery of the health PPP project and to obtain maximum value for money.
101chap7_p_101Specific rules for structuring procurement competitions for PPP projects should be set out in a local PPP or procurement law. However, the relevant law may not foresee every eventuality that might arise during the course of a procurement competition.
102chap7_p_102Procuring entities must, therefore, exercise individual discretion in some circumstances and, in doing so, must act in accordance with the general principles of transparency, equal treatment of tenderers and taking steps which are proportionate to the outcome to be achieved.
 chap7_img_5
chap7_img_5
Developing a Pipeline of Health PPP Projects
103chap7_p_103To plan health PPPs effectively, the public sector first needs a clear pipeline of priority projects. This begins with a health master plan that identifies the gap between the services people need and what the system currently provides. The master plan should utilise demographic and disease-burden data - both current and projected - to determine the types of facilities required, their optimal locations and the services they should offer. These may include primary care centres, diagnostic hubs, hospitals, rehabilitation facilities and palliative care services.
104chap7_p_104The planning process should consider how to optimise operations, such as reducing lengths of stay, incentivising preventive care, shifting to outpatient settings and increasing the use of day surgeries. These improvements reduce both capital and operating costs, the latter of which typically make up most of a facility’s budget. The master plan, for example, may highlight a need for a healthcare network in a specific region that includes improved preventive care and outreach models, rather than just a new hospital.
105chap7_p_105This analysis will produce a list of potential projects that governments should prioritise based on impact, cost and feasibility. Where conditions allow, selected projects can then be developed as PPPs using appropriate PPP models.
Preparation of Health PPP Projects
106chap7_p_106Each procuring entity will need to comply with the business case approval process applicable to their health PPP project. In addition to the key decisions required as part of the business case approval process, each procurement procedure requires a considerable amount of planning and preparation by the procuring entity before a tender notice can be advertised for the health PPP project.
107chap7_p_107The readiness of each procuring entity to commence procurement will be assessed as part of the consideration of the business case for their PPP project. The issues which will be evaluated include:
- chap7_ol_0
- chap7_li_76Clear scope for the health PPP project. Have the needs and requirements of the procuring entity been determined?
- chap7_li_77Governance arrangements for the PPP project. Has governance been adequately considered and resolved? Has an accountable line of responsibility been established to which the procurement team can report? Are all the responsible players named and committed to their roles? Each health PPP project requires an appropriately skilled and experienced procurement team that leads the procurement competition, supported by informed decision-makers. The governance hierarchy for decisions to be made during the procurement competition should be circulated to all decision-makers and those involved in evaluating tenderers.
- chap7_li_78Procurement documents (including the PPP contract). How advanced is the draft documentation? Have any applicable template documents and guidance issued by the PPP unit been used, and any derogations approved? Have the risks of the health PPP project been fully identified and allocated in the PPP contract?
- chap7_li_79Appropriate market sounding. Assessing the market (for example, through market research or direct engagement with potential tenderers) to determine whether the level of private sector interest is likely to be sufficient to ensure genuine competition is crucial.
- chap7_li_80Practical matters. Have issues such as the availability of internal resources, the appointment of external advisers and the provision of electronic procurement platforms been adequately considered and resolved?
108chap7_p_108The typical procurement pitfalls set out in the diagram below must be considered and avoided (where at all possible) by the procuring entity to ensure successful procurement and implementation of their health PPP project.
 chap7_img_6
chap7_img_6
Development of the Procurement Strategy for a Health PPP Project
109chap7_p_109Several public procurement decisions will need to be made early in respect of the procurement of health PPP projects. These decisions will influence not only the structure of each procurement competition and the content of the associated tender documentation, but also market perception and the procurement timetable. In all instances, the procurement strategy must be consistent with the principles of the applicable local policy, and an appropriate procurement team, with the necessary knowledge and mandate, will have been appointed. The following key decisions are required:
The Public Procurement Procedure
110chap7_p_110In each jurisdiction, there will be various types of procurement procedures for health PPP projects, which could include the open procedure, the restricted procedure, the negotiated procedure and competitive dialogue.
111chap7_p_111Generally speaking, open procedures are unsuitable for the procurement of complex financed PPP projects as they do not allow for the shortlisting of bidders and have no mechanism for dialogue or negotiation with tenderers.
112chap7_p_112Restricted procedures are generally designed as a one-step tender process. While a shortlist of tenderers may be invited to participate (following a Request for Qualification (RfQ)), there is only one round of tenders and no mechanism for dialogue, negotiation or down-selecting after pre-qualification. This procedure would be unsuitable for the procurement of PPP projects with a complex financing structure.
113chap7_p_113The negotiated procedure or competitive dialogue permits the shortlisting of tenderers at the RfQ stage, and negotiation or dialogue during the Request for Proposals (RfP) stage. Limited negotiation and clarification is usually also permitted under the competitive dialogue procedure (following submission of final tenders). Negotiated and competitive dialogue procedures are generally more appropriate for the procurement of health PPP projects because:
- chap7_ul_22
- chap7_li_81The needs of the procuring entity cannot be met without adaptation of readily available solutions.
- chap7_li_82The PPP contract includes design or innovative solutions.
- chap7_li_83The PPP contract cannot be awarded without prior negotiation due to specific circumstances related to its nature, complexity, legal and financial makeup or because of risks attached to it.
- chap7_li_84The technical specifications cannot be established with sufficient precision by the procuring entity.
Typical Structure for a Competitive Dialogue Procurement for a Health PPP Project
114chap7_p_114It is recommended that the competitive dialogue procedure for the procurement of health PPP projects should be structured in the following successive stages:
- chap7_ul_23
- chap7_li_85Preliminary market engagement
- chap7_li_86Advertisement
- chap7_li_87Prequalification and shortlisting
- chap7_li_88RfP issued to shortlisted tenderers
- chap7_li_89Dialogue period
- chap7_li_90Close dialogue and invitation to submit final proposals
- chap7_li_91Contract award
115chap7_p_115The diagram set out below illustrates the successive stages of a typical competitive dialogue procedure for a health PPP project.
 chap7_img_7
chap7_img_7
Shortlisting and Invitation of Bidders to the Procurement Competition
116chap7_p_116There will be procurement cost and time savings if fewer tenderers are shortlisted and invited to participate in the procurement competition for each health PPP project. However, there is a risk to competitive tension if fewer tenderers are shortlisted and subsequently a tenderer withdraws without submitting a final tender. It is recommended that three tenderers be shortlisted for each health PPP project. However, shortlisting more than three tenderers could be reviewed on a project-by-project basis, taking into account potential market changes.
Evaluation Criteria for Shortlisting Bidders to the Procurement Competition and Contract Award
117chap7_p_117Robust evaluation methodologies will be required for the shortlisting of bidders and the evaluation of tenders. In essence, shortlisting entails evaluating the economic and financial standing, as well as the professional/technical ability, of each bidder. Tender evaluation involves assessing the tenders received. Therefore, two sets of evaluation criteria will be required.
118chap7_p_118Tender Documents for a Health PPP Procurement Competition
119chap7_p_119There are two key tender documents for a health PPP procurement competition: the RfQ and the RfP. The purpose of the RfQ is to enable the procuring entity to identify suitably qualified and experienced tenderers who will be invited to participate in the procurement competition for the PPP project.
120chap7_p_120The RfQ should provide detailed information regarding the procuring entity’s requirements for the PPP project and arrangements. The RfQ is also an essential document for the private sector, as it enables potential tenderers to make an informed decision on whether to participate in the procurement competition.
121chap7_p_121The issue of the RfP represents a formal invitation from the procuring entity to tenderers to participate in dialogue or negotiation (where negotiated or competitive dialogue procedures are being used). The purpose of the RfP is to initiate and develop dialogue with the tenderers with a view to identifying the most advantageous tender.
122chap7_p_122The RfP should provide detailed information regarding the procuring entity’s requirements and arrangements for the conduct of the RfP stage of the procurement competition, including the submission of tenders and their evaluation.
Required Resources
123chap7_p_123Health PPP procurements require significant resourcing, both internally from the procuring entity’s personnel and externally from advisors, such as legal, financial, technical, clinical, equipment, insurance and environmental and social advisers. Roles and responsibilities for matters such as procurement, evaluation, contract negotiation and stakeholder engagement should be determined at the business case stage. A skills audit should be carried out to assess available in-house capabilities, any training requirements and the level of external support required.
Procuring Entity Project Team’s Role
124chap7_p_124Following the approval of the business case for a health PPP project, the procuring entity’s project team is responsible for:
- chap7_ul_24
- chap7_li_92Structuring the procurement competition and providing input to, and reviewing, the procurement documents (including the PPP contract).
- chap7_ul_25
- chap7_li_93Managing the RfQ process, including the clarifications process and notifying unsuccessful applicants, and evaluating RfQ responses.
- chap7_ul_26
- chap7_li_94Managing and participating in procurement competitions (including clarifications, dialogue and negotiations), and evaluating the tenders submitted.
- chap7_ul_27
- chap7_li_95Managing the contract award process (including notifying unsuccessful tenderers) and financial close.
- chap7_ul_28
- chap7_li_96Obtaining internal approvals for the health PPP project and managing other stakeholder requirements.
125chap7_p_125There must, therefore, be absolute clarity on the role and responsibilities of each member of the procuring entity’s project team.
126chap7_p_126Effective management of a procurement competition requires strict scoping of the timetable for the procurement competition, and for the procurement competition to be mapped from start to finish to allocate the necessary time and staffing resources. This is important in terms of identifying any pinch points where additional resources may be required.
127chap7_p_127An analysis must be conducted to determine the likely time commitment required from each member of the procuring entity’s project team. This will enable a procuring entity to determine whether its internal personnel (e.g. clinical, financial, technical, legal, estates, insurance/risk, etc.) should be part of the project team on a full-time basis or whether a more tailored approach using those personnel on an ad hoc basis with support from external advisors is more appropriate. In addition, thought should be given to ensuring continuity of personnel throughout the pre-procurement, procurement and contract management stages.
Duration of the Procurement Competition
128chap7_p_128The length of the procurement competition will depend on several factors, including the type of PPP being procured, the chosen procurement procedure and whether there is an urgent requirement for the procurement. Above all else, the procuring entity should not be pressured into accelerating the timescales for the procurement competition by senior officials. A typical DBFO procurement using the competitive dialogue procedure could take 18 to 24 months.
129chap7_p_129In terms of developing and applying the programme for the procurement competition, it is recommended that the following general principles be used for fixing time limits:
- chap7_ul_29
- chap7_li_97When receiving RfQ responses, pre-dialogue meeting deliverables, and tenders, procuring entities should consider the complexity of the health PPP project and the associated PPP contract.
- chap7_li_98When asked for time extensions, procuring entities should extend the time limits for the receipt of RfQ responses or tenders in the following cases:
- chap7_li_99Where additional information, although requested by the tenderer in good time, is not supplied by the procuring entity in a reasonable time before the time limit fixed for the receipt of RfQ responses or tenders.
- chap7_li_100Where significant changes are made to the tender documentation.
- chap7_ul_30
130chap7_p_130The length of the extension of time must be proportionate to the significance of the information or change. Where additional information has either not been requested promptly or its importance in preparing responsive tenders is insignificant, procuring entities do not need to extend the time limits.
Case Study: Getting the Timelines Wrong131chap7_p_131A healthcare PPP was well-structured and demonstrated strong feasibility during the feasibility study phase. However, in the subsequent procurement stage, insufficient time was allocated to assessing market appetite and effectively marketing the opportunity to potential investors. Compounding this, political pressure led the procuring authority to adopt overly ambitious timelines, including a compressed window for submission of RfQ responses. As a result, only one bidder submitted a response, forcing the procuring entity to reconsider its approach. |
Risk Allocation in Health PPP Projects
132chap7_p_132In a health PPP project, each risk should be allocated to the party best able to manage that risk. The provisions in the PPP contract should be drafted in such a way as to incentivise that party to mitigate such risk. Incentives could include performance or availability deductions, or damages and reliefs under the PPP contract.
133chap7_p_133If risk is not allocated effectively by the procuring entity in the PPP contract, unnecessary risk premiums will be levied by the private partner, meaning:
- chap7_ul_31
- chap7_li_101Less value for money for the public sector
- chap7_li_102Less market participation
- chap7_li_103Less effective competition
134chap7_p_134The approach to risk allocation varies by jurisdiction, and what may be a market norm in one country may not be in another. Additionally, different sectors have varying standards for risk allocation. The diagram below illustrates examples of typical PPP risks and health PPP risks.
 chap7_img_8
chap7_img_8
Choosing a Contractual Model for Health PPP
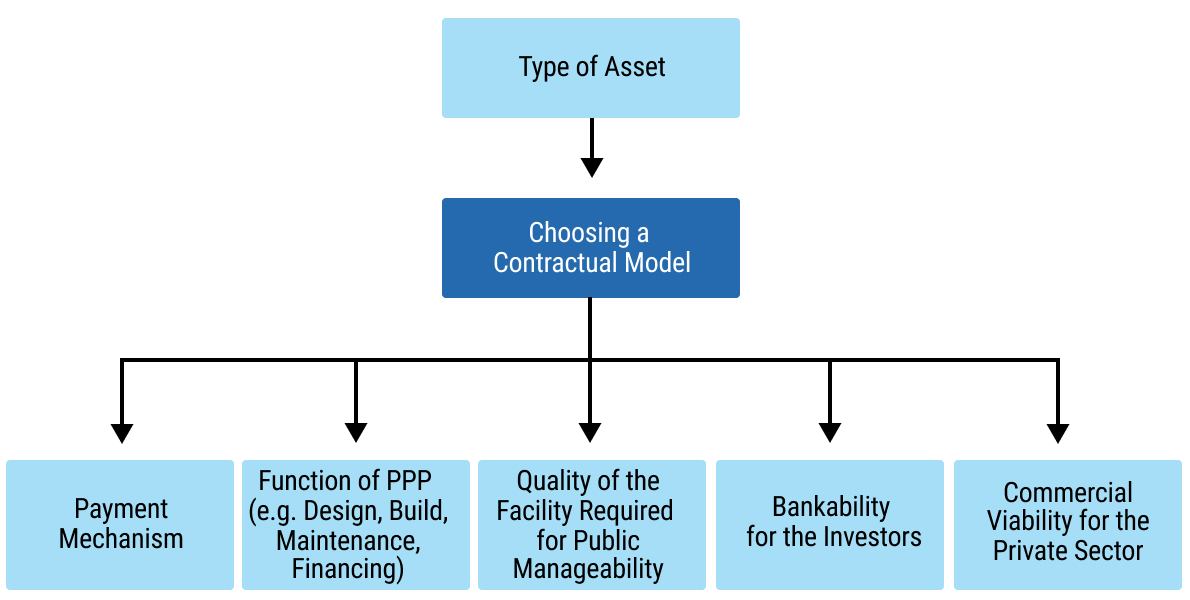
135chap7_p_135A range of different PPP contractual models can be used to deliver health PPP projects. Choosing the right contractual model involves considering several key factors, as illustrated in Figure 7.10 below.
 chap7_img_9
chap7_img_9
136chap7_p_136Table 7.2 below sets out a selection of the PPP contractual models which could be chosen for a health PPP.
|
137chap7_p_137PPP Contractual Model |
138chap7_p_138Type of Asset |
139chap7_p_139Overview |
140chap7_p_140Payment Source |
|
141chap7_p_141Management Contract |
142chap7_p_142Existing infrastructure |
143chap7_p_143The government retains ownership of assets and responsibility for capital expenditure. The private sector is responsible for maintenance and operation. Typically shorter in duration (3-10 years). |
144chap7_p_144Management fees are extended to the contractor |
|
145chap7_p_145Output-Based Performance Contract |
146chap7_p_146Existing infrastructure |
147chap7_p_147The private sector is provided with the freedom to meet performance requirements. |
148chap7_p_148Typically, the monthly fee from the government is based on performance indicators |
|
149chap7_p_149Build-Own-Operate- Transfer 150chap7_p_150(BOOT) |
151chap7_p_151New infrastructure |
152chap7_p_152Private sector builds, owns and maintains the asset for the duration of the contract. Handed back to the public sector upon termination or expiry of the contract. |
153chap7_p_153Government or user |
|
154chap7_p_154Build/Rehabilitate- 155chap7_p_155(BOT/ROT) |
156chap7_p_156New infrastructure |
157chap7_p_157The private sector builds or rehabilitates and maintains assets for the duration of the contract. Handed back to the public sector upon termination or expiry of the contract. |
158chap7_p_158Government or user |
|
159chap7_p_159Build-Own-Operate 160chap7_p_160(BOO) |
161chap7_p_161New infrastructure |
162chap7_p_162The private sector builds and maintains the asset for the duration of the contract. The asset is not handed back to the public sector. |
163chap7_p_163Government or user |
|
164chap7_p_164Design-Build-Finance-Operate 165chap7_p_165(DBFO) |
166chap7_p_166New infrastructure |
167chap7_p_167The private sector designs, builds, finances, operates and maintains an asset, then leases it back to the government (typically for 25-30 years). |
168chap7_p_168Government or user |
|
169chap7_p_169Build, lease, transfer 170chap7_p_170(BLT) |
171chap7_p_171New infrastructure |
172chap7_p_172The private sector builds and leases the asset back to the government. Handed back to the public sector upon termination or expiry of the contract. |
173chap7_p_173Government 174chap7_p_174or user |
|
175chap7_p_175Concession |
176chap7_p_176New or existing infrastructure |
177chap7_p_177Varies depending on the jurisdiction, but typically, a grant by a government of the right to provide a service or use an asset. |
178chap7_p_178User |
 chap7_img_10
chap7_img_10
179chap7_p_179To further assist in selecting the right PPP contractual model for a health PPP project, the appraisal criteria and considerations outlined in Table 7.3 below should be applied.
|
180chap7_p_180Appraisal Criteria |
181chap7_p_181Considerations |
|
182chap7_p_182Accessibility of Public Medical Services |
183chap7_p_183The potential for the PPP model to provide health care and services to patients (including patients who may not be insured or able to pay for medical care). |
|
184chap7_p_184Quality of the Project |
185chap7_p_185The potential for the PPP model to deliver a good quality project, resulting in a positive experience for patients and staff. |
|
186chap7_p_186Manageability of the Project |
187chap7_p_187The potential for the PPP model to be within the capability of the procuring entity to effectively administer, including (i) management and delivery of the procuring entity’s responsibilities in the PPP contract, and (ii) ensuring that the private partner is effectively managed in accordance with the terms of the PPP contract. |
|
188chap7_p_188Potential for Better Value-for-Money |
189chap7_p_189The potential for the PPP model to offer a good combination of price and quality risk in the delivery and operation of the PPP project. |
|
190chap7_p_190Potential for Lifecycle Optimisation |
191chap7_p_191The potential under the PPP model is that the design and construction of the PPP project can be optimised to present the best value over the lifetime of the PPP project. |
|
192chap7_p_192Leveraging Key Private Sector Capabilities |
193chap7_p_193The extent to which the private sector will be capable of being involved in, and performing its required role under, the PPP model. |
|
194chap7_p_194Commercial Viability of the PPP Project for the Private Sector |
195chap7_p_195Will there be sufficient commercial potential and interest for private operators (and investors) in the PPP model? |
|
196chap7_p_196Bankability for Investors |
197chap7_p_197The extent to which the PPP model will allow for the provision of sufficient (debt) financing. |
|
198chap7_p_198Potential for Competitive Procurement |
199chap7_p_199Whether the PPP model will allow for sufficient competition in the procurement. |
The Health PPP Project Agreement
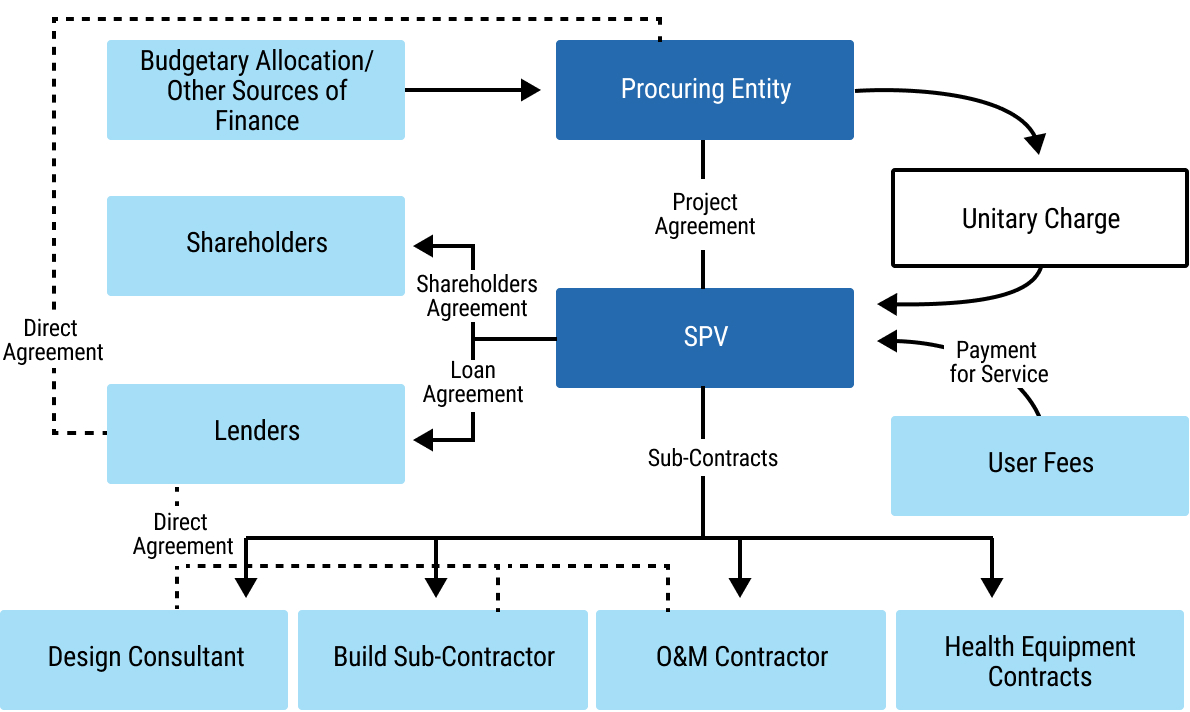
200chap7_p_200The PPP contract, also known as the project agreement, is the key contract that the procuring entity is required to enter into with the private partner, in connection with, for example, the DBFO of the health PPP project being procured. Figure 7.12 below illustrates the location of the project agreement within a DBFO contractual model, as well as the key contracting parties and other contracts that form part of the DBFO contractual model.
 chap7_img_11
chap7_img_11
201chap7_p_201The project agreement should be developed by the procuring entity prior to the commencement of the procurement competition and will then be the subject of dialogue or negotiation (in the context of a competitive dialogue or negotiated procurement procedure) between the procuring entity and tenderers.
202chap7_p_202The development of the project agreement should reflect the outcome of the risk identification and allocation process, which should have been undertaken with respect to the health PPP project. In addition to the normal matters which are considered in the development of a project agreement (e.g. grounds for termination and compensation on termination, dispute resolution, force majeure and land issues, amongst many others), key issues for the development of a project agreement for a health PPP include consideration of:
- chap7_ul_32
- chap7_li_104Maintenance. Does the scope of the project agreement include soft facilities management (soft FM) and hard facilities management (hard FM) or just hard FM? Hard FM relates to the physical aspects of buildings. This means that any service carried out on a bodily structure falls under hard FM. Often, hard FM services are required by law to ensure that facilities are safe for staff, patients and any visitors. Hard FM services include: fire safety services, gas maintenance, plumbing, heating, ventilation, air conditioning, building maintenance, electrical and lighting maintenance and accessibility maintenance. Soft FM relates to services which ensure buildings maintain a secure and pleasant environment. Soft FM services include waste management, cleaning services, grounds maintenance and landscaping, security services, catering, pest control and janitorial services.
- chap7_li_105Technological change. Suppose health equipment is part of the scope for the PPP contract. In that case, the contract must include mechanisms to adapt to rapid technological and medical advancements, such as new equipment or treatment protocols.
- chap7_li_106Epidemic/pandemic response. Specific clauses defining roles, responsibilities and financial implications in the event of a public health crisis (e.g. pandemic response) should be included, ensuring seamless integration into national emergency plans.
- chap7_li_107Interoperability. When the provision of information technology (IT) systems is included in the scope of the PPP contract, consideration should be given to ensuring that the private partner’s IT systems are compatible and interoperable with existing national or regional health information systems, thereby facilitating continuity of care and public health monitoring.
- chap7_li_108Data sharing and ownership. Clearly, healthcare generates sensitive patient data. If the private partner will have access to patient data, there should be explicit clauses regarding data ownership, privacy, security and protocols for sharing data with public health authorities.
- chap7_li_109Output-oriented specifications. If appropriate, the scope of the PPP contract should move beyond merely specifying infrastructure (e.g. number of beds) to defining the desired health outcomes (e.g. healthcare-associated infection rates, readmission rates, wait times).
- chap7_li_110Patient safety and risk management. Clear protocols for identifying, managing and reporting clinical risks and incidents should be included in the PPP contract.
- chap7_li_111Clinical effectiveness and audit. Mandating regular clinical audits against national and local standards to ensure best practices are followed should be included in the PPP contract.
- chap7_li_112Stakeholder engagement. Provisions in the PPP contract should outline communication and engagement processes between the public partner, private partner, healthcare professionals and patient representatives to foster trust and proactively manage issues.
Management of the PPP Contract
203chap7_p_203The procuring entity is responsible for ensuring that a PPP contract is administered correctly and enforced in accordance with its terms and conditions. For this purpose, it is recommended that the procuring entity:
- chap7_ol_1
- chap7_li_113Establishes a contract management team which will oversee the administration of the PPP contract. Ideally, this team should include personnel who have been involved in the procurement of the health PPP project.
- chap7_li_114Provides the necessary resources, including human resources, to its contract management team to enable effective contract administration,
- chap7_li_115Appoints where required, technical, financial and legal experts as members of the procuring entity’s contract management team to assist with any aspect of the administration or enforcement of the PPP contract, which may include:
- chap7_li_116In respect of the legal expert, interpretation of the terms and conditions of the PPP contract, variations of the PPP contract, termination of the PPP contract and disputes in connection with the PPP contract.
- chap7_li_117In respect of the financial expert, operation of the payment mechanism, audit and accounting regarding the PPP contract, variations of the PPP contract and the operation of performance guarantees.
- chap7_li_118In respect of the technical expert, design and construction, completion and commissioning, defects rectification, operation and maintenance, variations of the PPP contract and handback and transfer issues.
- chap7_ul_33
204chap7_p_204The procuring entity, supported by its contract management team, should establish procedures for the administration of each PPP contract, and these should include:
- chap7_ol_2
- chap7_li_119Managing governance of the PPP contract (which should include a process for the recording and communication of the appropriate decision-making authorities in respect of the PPP contract).
- chap7_li_120Communicating and liaising with the private partner (which should include the preparation of a comprehensive communications plan) and any independent engineer or third party who has been appointed pursuant to the PPP contract.
- chap7_li_121Monitoring, evaluating and regulating the performance by the private partner of the PPP contract and the implementation of the health PPP project by the private partner (which should include the preparation of a comprehensive contract management plan).
- chap7_li_122Measuring outputs related to the performance of the private partner in terms of the PPP contract, including the involvement in such measurement by any independent engineer or third party who has been appointed pursuant to the PPP contract.
- chap7_li_123Receiving, reviewing and addressing issues arising from reports submitted by the private partner to the procuring entity pursuant to the PPP contract.
- chap7_li_124The provision of reports by the private partner to the procuring entity in respect of the health PPP project and its progress, including but not limited to achievements, challenges, obstacles and outstanding issues.
- chap7_li_125Ensuring that all rectification measures are undertaken by the private partner on a timely basis and performance regimes are strictly and timeously enforced in accordance with the PPP contract.
- chap7_li_126Management responsibilities including managing stakeholder engagement, managing any variation, termination or dispute, managing transfer or handback of the health PPP project and managing accounting, audit and other compliance and regulatory matters.
205chap7_p_205Where relevant in the context of the type of health PPP project, it is recommended that the procuring entity, supported by its contract management team, establishes a procedure for the transfer or handback of the asset comprised in the PPP project on the occurrence of the date of expiry of the PPP contract. Such a procedure should ensure that the asset is handed back or transferred to the procuring entity in a condition which is in accordance with the terms of the PPP contract, with the required documentation for the procuring entity or another private partner to manage and operate the asset. Such a procedure may also include:
- chap7_ul_34
- chap7_li_127Joint inspection by the procuring entity and the private partner to assess the condition of the asset before transfer or handback.
- chap7_li_128Pursuant to such joint inspection, identification of any remedial measures which need to be taken by the private partner (at the private partner’s cost) before the asset is transferred or handed back to the procuring entity.
206chap7_p_206The procuring entity should also give consideration regarding its reporting obligations under law (or procedure) to other public entities (e.g. PPP unit, audit office). Reports could include details with respect to:
- chap7_ol_3
- chap7_li_129The relevant project and its progress.
- chap7_li_130Any achievements of the procuring entity in respect of the PPP project.
- chap7_li_131Any challenges or obstacles which the procuring entity has encountered in respect of the PPP project, and how the procuring entity dealt with those challenges or obstacles.
- chap7_li_132Any outstanding issues in respect of the PPP contract and how the procuring entity plans to deal with those outstanding issues.
- chap7_li_133The performance of the private partner as measured against the requirements of the PPP contract.
- chap7_li_134Any variations or disputes under the PPP contract.
- chap7_li_135Any preparations for transfer or handback of the PPP project.
- chap7_li_136Any local development opportunities and any community involvement (e.g. support to local businesses, technology or skills transfer, job creation).
Case Study: Failure of the Government to Deliver its Obligations Under the PPP Contract207chap7_p_207A government procured specialised medical equipment under a PPP arrangement for public hospitals across the country. The installation of the equipment requires prerequisite works at the beneficiary facilities, including an adequate water supply, three-phase power and other necessary infrastructure upgrades to meet the specified technical standards. 208chap7_p_208However, several facilities were not adequately equipped to meet these requirements and lacked the necessary funding to undertake the preparatory works. Consequently, the contractors were unable to install the equipment as scheduled, resulting in significant portions of the equipment remaining in storage for extended periods while the facilities sought to upgrade their infrastructure. 209chap7_p_209During this period, the contractors continued to be entitled to availability payments, as the delay in equipment installation was attributable to the public entities. As a result, the public sector incurred financial obligations without the corresponding service benefits and the intended health outcomes and value-for-money objectives of the PPP. 210chap7_p_210A key lesson from this experience is that procuring entities must be fully prepared to fulfil their obligations under any PPP contract. In this case, a robust contract management team could also have helped anticipate potential performance issues, ensuring that the PPP delivered its full intended value. |