
Search in the book
Crédits photographiques
intercalaire 1 pour la démo
Table des matières
Cat. 1
cat1_h4_0Historique
Ce tableau fut commencé vers 1503 au moins, sans doute pour Francesco del Giocondo, gentilhomme florentin (1460-1539), mais fut conservé par Léonard de Vinci jusqu’à la fin de sa vie pour en pursuivre l’exécution picturale toujours inachevée à sa mort ; il fut très probablement acquis par François Ier en 1518[1].
cat1_h4_1Bibliographie
Brejon de Lavergnée et Thiébaut, 1981, p. 192, ill. ; Habert et Scailliérez, 2007, p. 61-122, p. 81, ill. n&b ; Delieuvin et Franck, 2019, p. 224-233.
1cat1_p_1Si l’on nous demande pourquoi figure, dans cet ouvrage consacré au Louvre, un tableau qui ne s’y trouve plus, nous répondrons que la disparition même de l’admirable Joconde nous la rend encore plus chère et nous fait désirer davantage de la pouvoir contempler, ne fût-ce qu’en effigie.
2cat1_p_2On n’a pas oublié l’émotion qui secoua l’univers civilisé lorsque se répandit l’incroyable nouvelle : « La Joconde a été volée. » Sur tous les points du globe, cette perte fut ressentie comme un désastre. Désastre, certes, et sans équivalent, car, avec la Joconde, a disparu l’une des plus grandioses productions du génie humain. Malgré son prodigieux assemblage de chefs-d’œuvre, le Salon Carré a perdu le meilleur de sa gloire ; dans l’écrin rempli de joyaux manque le plus beau diamant, celui qui jetait les feux les plus brillants et les plus purs. La Mona Lisa n’accueille plus le visiteur de son sourire énigmatique et qui sait en quels lieux l’étrange créature repose aujourd’hui son troublant et mystérieux regard ? Et, malgré tout, survit en nous l’indéfectible espérance de la revoir un jour à son ancienne place, triomphante et narquoise, et groupant une cour encore plus nombreuse d’adorateurs autour de son immortelle beauté.
3cat1_p_3Nulle peinture au monde n’a provoqué une aussi entière admiration. La Joconde a eu ses poètes, ses romanciers, ses amants. Certains hommes l’ont adorée comme un être vivant ; il en est même qui se sont tués pour elle et peut-être faut-il chercher dans une passion de cet ordre l’énigme de son étrange disparition.
4cat1_p_4Relisons la page enthousiaste où Théophile Gautier célèbre la Mona Lisa[2] :
5cat1_p_5« La Joconde ! Sphinx de beauté qui souris si mystérieusement dans le cadre de Léonard de Vinci et sembles proposer à l’admiration des siècles une énigme qu’ils n’ont pas encore résolue, un attrait invincible ramène toujours vers toi ! Oh ! en effet, qui n’est resté accoudé de longues heures devant cette tête baignée de demi-teintes crépusculaires, enveloppée de crêpes transparents et dont les traits, mélodieusement noyés dans une vapeur violette, apparaissent comme une création du Rêve à travers la gaze noire du Sommeil ! De quelle planète est tombé, au milieu d’un paysage d’azur, cet être étrange avec son regard qui promet des voluptés inconnues et son expression divinement ironique ? Léonard de Vinci imprime à ses figures un tel cachet de supériorité qu’on se sent troublé en leur présence. Les pénombres de leurs yeux profonds cachent des secrets interdits aux profanes et les inflexions de leurs lèvres moqueuses conviennent à des dieux qui savent tout et méprisent doucement les vulgarités humaines.
6cat1_p_6Quelle fixité inquiétante et quel sardonisme surhumain dans ces prunelles sombres, dans ces lèvres onduleuses comme l’arc de l’Amour après qu’il a décoché le trait ! Ne dirait-on pas que la Joconde est l’Isis d’une religion cryptique qui, se croyant seule, entr’ouvre les plis de son voile, dût l’imprudent qui la surprendrait devenir fou et mourir ? Jamais l’idéal féminin n’a revêtu de formes plus inéluctablement séduisantes. Croyez que si don Juan avait rencontré la Mona Lisa, il se serait épargné d’écrire sur sa liste trois mille noms de femmes ; il n’en aurait tracé qu’un, et les ailes de son désir eussent refusé de le porter plus loin. Elles se seraient fondues et déplumées au soleil noir de ces prunelles. Nous l’avons revue bien des fois, cette adorable Joconde, et notre déclaration d’amour ne nous paraît pas aujourd’hui trop brûlante. Elle est toujours là, souriant avec une moqueuse volupté à ses innombrables amants. Sur son front repose cette sérénité d’une femme sûre d’être éternellement belle et qui se sent supérieure à l’idéal de tous les poètes et de tous les artistes. »
7cat1_p_7Le divin Léonard mit quatre ans à faire ce portrait, qu’il ne pouvait se décider à quitter et qu’il ne considéra jamais comme fini ; pendant les séances, des musiciens jouaient pour égayer le beau modèle et empêcher ses traits charmants de prendre un air d’ennui et de fatigue.
8cat1_p_8Doit-on regretter que le noir particulier qu’employait Léonard ait prévalu dans les teintes de la Mona Lisa et leur ait donné cette délicieuse harmonie violâtre, cette tonalité abstraite qui est comme le coloris de l’idéal ? Nous ne le pensons pas. Maintenant, le mystère s’ajoute au charme et le tableau, dans sa fraîcheur, était peut-être moins séduisant.

9cat1_p_9Le modèle de ce magnifique portrait s’appelait Lisa Maria di Noldo Gherardini ; elle épousa, en 1495, Francesco di Bartolomeo de Zenobi del Giocondo, d’où son nom de « Joconde », sous lequel elle est aujourd’hui célèbre (Fig. 1-1).
10cat1_p_10La Joconde fut peinte vers 1500. François Ier l’acquit pour quatre mille écus d’or et la fit placer dans le cabinet doré de Fontainebleau. Elle passa ensuite dans la chambre de Louis XIV, à Versailles. Après la Révolution, le célèbre portrait fut transporté au Louvre et placé dans le Salon Carré, d’où il disparut en août 1911.
11cat1_p_11Hauteur : 0.77. – Largeur : 0.53. – Figure en buste grandeur nature.
Voir sur le site des collections du musée du Louvre https://collections.louvre.fr/ark:/53355/cl010062370 : « Données historiques ».
Gautier, 1882, chapitre « Salon Carré », p. 26. Consulter l’ouvrage sur la bibliothèque numérique de l’Institut national d’histoire de l’art : https://bibliotheque-numerique.inha.fr/collection/item/8352-guide-de-lamateur-au-muse-du-louvre.
Cat. 2
cat2_h4_0Historique
Commandé par Charles Ier d’Angleterre (?) pour remplacer un portrait de la reine Anne, par Paul Van Somer (1617), au château d’Oatlands (?)[1] ; la dispersion des collections royales britanniques, puis leur histoire au long du xviie siècle, font perdre la trace du tableau[2] ; […] ; 13 juillet 1797 : le tableau est inventorié par les commissaires révolutionnaires, à Versailles, dans la chambre de la reine ; 15 juillet 1797 : envoyé au Muséum central des arts (dans un lot expédié en échange du « cloître des Chartreux et [d]es ports de Vernet[3] ») ; 5 août 1797 : récépissé de l’arrivée des œuvres donné à Fragonard « chargé par le Ministre de l’intérieur de surveiller les transports[4]14 » ; 1816 : les experts du musée l’estiment 100 000 francs[5] ; 17 juillet 1945 : retour du château de Montal après évacuation pendant la Seconde Guerre mondiale[6].
cat2_h4_1Bibliographie
Dezallier d’Argenville, 1752, p. 415 ; Rumberg et Shawe-Taylor, 2018, no 76, p. 7, 22, 131, 244, et note 41, p. 257 ; Ayres, 2020, paragraphe 16 et fig. 11 ; White, 2021, p. 222-224 et fig. 203 ; Eaker, 2022, p. 109 et fig. 52 p. 111 ; Ducos, 2023, no 18 (https://livres.louvre.fr/vandyck/cats/18/).
1cat2_p_1LE portrait de Charles Ier d’Angleterre, que possède le Louvre, est un chef-d’œuvre légendaire.
2cat2_p_2Le poing sur la hanche, du côté de l’épée, la main droite appuyée sur une haute canne, le roi tourne légèrement sa tête fine et blonde, encadrée d’un grand chapeau. Il regarde avec calme, avec assurance, et toute son attitude est celle d’un homme habitué à commander. Sa veste de soie grise est traversée du baudrier qui soutient l’épée. Au-dessous de la culotte rouge et laissant voir les bas de soie, des bottes souples en cuir fauve, garnies d’éperons, emprisonnent une jambe nerveuse et élégante. Un peu en arrière, le cheval favori du roi piaffe, impatient, maintenu par un écuyer vêtu de rouge qui représente le chevalier d’Hamilton ; un autre serviteur, plus loin, porte le manteau du souverain. Le tertre où sont placés les personnages est ombragé par la ramure épaisse d’un arbre et, sur les plans éloignés, s’étend une plaine au-dessus de laquelle des nuages gris floconnent dans le ciel bleu.

3cat2_p_3Ce tableau, d’une admirable composition, rend à merveille l’élégante silhouette de Charles Ier, le plus beau des Stuarts (Fig. 2-1). L’œuvre se présente avec une noblesse contenue, une richesse sourde et éclatante tout à la fois, une somptuosité discrète qui impressionnent, où l’on retrouve quelque chose de la manière de Rubens, mais tempérée, assagie, comme disciplinée.
4cat2_p_4Van Dyck avait d’ailleurs longtemps travaillé avec Rubens, qui l’appelait « le meilleur de ses élèves ». Son amitié lui fut aussi profitable que ses leçons. C’est lui qui le recommanda à la cour des Stuarts. Charles Ier, influencé par les éloges de Rubens pour son élève et ravi du portrait de Nicolas Lanière, son maître de chapelle, peint par Van Dyck, invita celui-ci à se rendre auprès de lui.
5cat2_p_5Van Dyck arriva à Londres et se présenta au roi qu’il conquit dès la première entrevue. Il avait une beauté fine, assez semblable à celle de Charles Ier, des manières aisées, une certaine grâce cavalière et l’air vif et dégagé d’un homme du monde accompli. Sa conversation n’était pas moins agréable que sa personne ; il avait la parole abondante et brillante, alimentée par un savoir profond et disciplinée par un tact infini. Le roi se plaisait beaucoup en sa compagnie ; il se rendait fréquemment à son atelier et, dépouillant avec lui toute contrainte d’étiquette, ils s’entretenaient ensemble de mille sujets pendant que Van Dyck travaillait à son portrait. De cette époque datent les nombreuses effigies du roi et de la reine.
6cat2_p_6En récompense de son talent, Van Dyck reçut le titre de principal peintre ordinaire de Leurs Majestés, fut créé chevalier et eut son logement à Blackfriars.
7cat2_p_7Dans son portrait de Charles Ier, Van Dyck s’était révélé portraitiste de génie et il n’est pas étonnant que, voulant suivre l’exemple du souverain, toute la noblesse enviât l’honneur de poser devant le grand artiste flamand. Bientôt, il ne put suffire aux commandes, il dut prendre des collaborateurs chargés de peindre les accessoires, se réservant seulement les têtes et les mains. Le succès venu, il eut toute liberté d’augmenter ses prix et gagna des sommes considérables qu’il dépensait largement. Sa maison était montée sur un pied magnifique, il possédait un équipage nombreux et élégant et offrait si bonne chère que peu de princes étaient aussi visités et aussi bien servis que lui.
8cat2_p_8En 1639, il épousa Mary Ruthven, demoiselle d’honneur de la reine, petite-fille de lord Ruthven, dont il eut une fille. Sa femme ne lui apportait pas de dot, mais elle était considérée comme une des plus merveilleuses beautés de son temps. Cette union fut de courte durée. Sa vie de travail et de plaisirs avait miné la santé de Van Dyck et malgré que Charles Ier eût promis trois cents livres au médecin s’il le sauvait, le grand peintre mourut à Blackfriars, le 9 décembre 1641, âgé seulement de quarante-deux ans.
9cat2_p_9« Non moins coloriste que Rubens, écrit Théophile Gautier, mais plus fin, plus élégant que son maître, Van Dyck semble créé pour peindre les rois, les princes, les duchesses, tout ce monde de la haute vie, fin de race, aristocratique d’allure, d’une magnificence héréditaire et marchant au-dessus de la multitude comme les dieux marchent sur les nuages. Il a peint d’une touche aisée et noble, avec une couleur brillante mais vigoureuse et une pénétration rapide du caractère, des têtes qu’on ne reverra plus, des masques dont le moule est brisé, des expressions d’existences à jamais évanouies.[7] »
10cat2_p_10Le portrait de Charles Ier entra dans le domaine national d’assez curieuse façon. À la vente du comte de Thiers, qui en était possesseur, la comtesse Du Barry l’acheta pour une somme de 24.000 livres. Et comme on lui demandait pourquoi elle avait choisi ce tableau de préférence aux autres de la collection qui semblaient devoir mieux lui convenir, elle répondit que c’était un portrait de famille, car elle prétendait tenir de la maison des Stuarts. Plus tard, elle le céda au même prix à M. d’Angivillers, pour le compte du Roi.
11cat2_p_11Ce tableau occupe aujourd’hui au Louvre la salle Van Dyck qui précède la nouvelle salle des Rubens.
12cat2_p_12Hauteur : 2.72. – Largeur : 2.12. – Figures en pied grandeur naturelle.
Rumberg et Shawe-Taylor, 2018, p. 22 : il s’agit là d’une hypothèse formulée par Per Rumberg et Desmond Shawe-Taylor, mais sur laquelle revient celui-ci (ibid., p. 131) et celui-là (ibid., no 76, p. 244). Voir aussi Millar, 1982, p. 21, pour le précédent, thématique, d’Henriette Marie partant pour la chasse. Ayres, 2020, paragraphe 16, s’appuyant sur Liedtke, 1989, p. 256-257, reprend l’idée suivant laquelle le tableau du Louvre serait le pendant du Portrait d’Anne de Danemark par Paul Van Somer (collection de S. M. la reine Élisabeth II, RCIN 405887). Les œuvres, en effet, sont de dimensions proches et le fils répondrait ainsi à la mère. Cette remarque a l’intérêt de rappeler l’importance possible de la figure maternelle dans les choix de Charles Ier. La difficulté, que ne souligne pas Sara Ayres, est évidemment que le Van Dyck relègue au rang d’image archaïque et dépassée le Van Somer, en cela parfaitement en accord avec la « procédure vandyckienne » habituelle de relégation à une classe inférieure des créations de différents artistes nordiques l’ayant précédé. Le cas de Daniel Mytens est le plus connu ; on peut aussi penser à l’esthétique de Michiel Van Mierevelt à La Haye. Que le Van Somer et le Van Dyck soient de dimensions très proches signifie peut-être simplement que Van Dyck, s’inscrivant dans une tradition, souhaitait susciter la comparaison, en sa faveur, avec l’œuvre, somme toute assez gauche, de son prédécesseur à la cour Stuart.
On reconnaît la Vie de saint Bruno, par Eustache Le Sueur, et la série des ports de France, par Joseph Vernet.
Cantarel-Besson, 1992, p. 124. Jean Honoré Fragonard, membre du conservatoire des Arts depuis janvier 1794 (grâce à l’intervention de Jacques Louis David) et chargé de l’administration du Muséum, se voit confier durant l’été 1797 le déménagement des œuvres (comme la mise en place du musée de l’École française à Versailles). Voir Martial Guédron, « Fragonard, Jean Honoré », Allgemeines Künstlerlexikon (2019), https://www-degruyter-com.bnf.idm.oclc.org/database/AKL/entry/_00069426/html, consulté le 30 mai 2020.
Voir Ducos, 2023, cat. 18, https://livres.louvre.fr/vandyck/cats/18, « Historique ».
Gautier, 1882, chapitre « Écoles allemande, flamande et hollandaises », p. 159. Consulter l’ouvrage sur la bibliothèque numérique de l’Institut national d’histoire de l’art : https://bibliotheque-numerique.inha.fr/collection/item/8352-guide-de-lamateur-au-muse-du-louvre.
Cat. 3
cat3_h4_0Historique
Vente « d’une riche collection d’articles curieux de tout genre » [Lespinasse d’Arlet], Paris, maison des divisions supplémentaires du Mont-de-Piété, 45 rue Vivienne, 11 juillet1803, organisée par Paillet et Delaroche, lot 335 : « Un très beau Tableau peint au pastel, par le célèbre Latour. Il représente Madame de Pompadour, de grandeur naturelle, en pied et assise, tenant un Livre de musique, et près d’un bureau où sont posés des Livres et autres accessoires. Ce morceau, le plus grand Ouvrage de cet Artiste, est recouvert par une belle Glace blanche faite exprès à Saint Gobain, et a appartenu à feu Louis XV. » Le portrait est à cette occasion acquis par Alexandre Joseph Paillet (1743-1814), l’un des deux organisateurs de la vente, pour la somme de 500 francs, et aussitôt revendu au Musée central des Arts[1].
cat3_h4_1Bibliographie
Salmon, 2018, cat. 90, p. 182-191 ; Ribeiro, 2020, p. 174-177, fig. 2 p. 175, note 4 p. 177.

1cat3_p_1Quentin La Tour fut un admirable pastelliste et un grand magicien de la couleur, la nature l’avait moins heureusement doté sous le rapport du caractère. Il était habituellement quinteux et fantasque. Très avancé dans les doctrines des Encyclopédistes, il affectait avec les grands une désinvolture frisant l’impertinence. On le voit reprocher au Dauphin que ses enfants sont fort mal élevés et qu’il se laisse duper par des fripons. Le roi lui-même doit subir ses boutades : pendant une séance de pose (Fig. 3-1), il fatigue Louis XV par un éloge outré des étrangers :
2cat3_p_2– Mais je vous croyais Français, lui dit le roi surpris. – Non, sire, répond hargneusement La Tour, je suis Picard, de Saint-Quentin.
3cat3_p_3L’exécution du portrait de Mme de Pompadour, notamment, est marquée de péripéties et d’incidents sans nombre. Quentin La Tour n’aime pas la favorite. De premières ouvertures lui sont faites en 1750, il les repousse ; prié de se rendre à Versailles auprès de la marquise, il se contente de répondre à l’envoyé :
4cat3_p_4– Dites à Madame que je ne vais pas peindre en ville.
5cat3_p_5Mme de Pompadour, dépitée, en écrit à son frère, le marquis de Marigny, qui est lié avec l’artiste. Son intervention amène un rapprochement et La Tour jette sur le papier deux préparations de son tableau. Puis il reste deux ans sans y travailler ; tous les prétextes lui sont valables pour se dérober. A Marigny qui le presse il écrit qu’il se sent en proie « à un abattement, à un anéantissement qui lui font craindre la fièvre », et il veut essayer « si l’air lui fera du bien ». Marigny se fâche alors, mais sans plus de résultat. Mme de Pompadour, qui tient à son portrait, essaye de la douceur : « Je suis, lui mande-t-elle, à peu près dans le même embonpoint où vous m’avez vue à la Muette et je crois qu’il serait à propos de profiter du moment pour finir ce que vous avez si bien commencé. Si vous pouvez venir demain, je serai libre et avec si peu de monde que vous voudrez. Vous connaissez, Monsieur, le cas que je fais de vous et de vos admirables talents. »
6cat3_p_6Vaincu par tant d’insistance, La Tour cède enfin et se rend à Versailles, sur la promesse qu’aucun fâcheux ne viendra interrompre le travail. Mais, en bon philosophe, il est bien résolu à « donner une leçon à ces gens-là ». Dès que la marquise est installée, il se met à son aise, enlève les boucles de ses escarpins, son col, sa perruque, ses jarretières et se coiffe d’un bonnet de taffetas. Survient le roi :
7cat3_p_7– Vous aviez promis, madame que votre porte serait fermée. – Je ne vous dérangerai pas, fait le roi souriant ; je vais rester là bien tranquille. Continuez. – Il ne m’est pas possible d’obéir à Votre Majesté ; je reviendrai lorsque madame sera seule : je n’aime point à être interrompu. Et il s’en fut.
8cat3_p_8Enfin, après trois ans d’efforts et de mécomptes, le portrait fut achevé et figura au Salon de 1855. Malgré l’évidente mauvaise volonté mise par La Tour à peindre la favorite royale, les témoignages du temps s’accordent à reconnaître qu’il mit de la galanterie à l’embellir. Combien différente et plus véridique est la « préparation » du tableau, qui se trouve aujourd’hui au musée de Saint-Quentin !
9cat3_p_9Mais, en dépit de son exécution volontairement flatteuse, ce portrait n’en est pas moins une œuvre de premier ordre, l’une des meilleures de La Tour. Sainte-Beuve lui a consacré une de ses pages les plus brillantes :
10cat3_p_10« C’est la personne même, écrit-il, qui est de tout point merveilleuse de finesse, de dignité suave et d’exquise beauté. Tenant en main le cahier de musique avec légèreté et négligence, elle est tout à coup distraite. Elle semble avoir entendu du bruit et retourne la tête. Est-ce bien le roi qui vient et qui va entrer? Elle a l’air d’attendre avec certitude et d’écouter avec sourire. Sa tête ainsi détournée laisse voir le profil du cou dans toute sa grâce et ses petits cheveux très courts, délicieusement ondés, dont les boucles s’étagent et dont le blond se devine encore sous la demi-poudre qui les couvre à peine. La tête nage dans un fond bleuâtre qui, en général, est celui de tout le tableau. L’œil est partout satisfait et caressé ; c’est de la mélodie plus encore que de l’harmonie. Il n’est rien dans ce boudoir enchanté qui ne semble faire sa cour à la déesse. Elle-même a les chairs et le teint d’un blanc lilas, légèrement azuré. Ce sein, ces rubans, cette robe, tout cet ensemble se marie harmonieusement. Tout dans la physionomie, dans l’attitude, exprime la grâce, le goût suprême, l’affabilité et l’aménité plutôt que la douceur, un air de reine qu’il a fallu prendre, mais qui se trouve naturel et se soutiendra sans trop d’efforts.[2] »
11cat3_p_11Mme de Pompadour se déclara satisfaite du pastel, mais quand vint l’heure du règlement, les difficultés recommencèrent. La Tour ne demandait rien moins que quarante-huit mille livres ! Après bien des pourparlers et des tiraillements, il dut se contenter de la moitié de cette somme, mais il ressentit de cette déconvenue une colère qui fut très longue à s’apaiser.
12cat3_p_12Le portrait de Mme de Pompadour passa, on ne sait comment, entre les mains du comte de Lespinasse d’Arlet, puis fut acquis, en 1797, par le Muséum des Arts. Il resta dans la poussière des réserves nationales jusqu’en 1838, date à laquelle il fut transféré au Louvre, où il figure aujourd’hui dans la salle des Pastels.
13cat3_p_13Hauteur : 1.70. – Largeur : 1.20. – Figure grandeur naturelle.
Voir sur le site des collections du musée du Louvre : https://collections.louvre.fr/ark:/53355/cl020213445 : « Données historiques ».
Bibliographie
Index
C
1indexcontenu_p_1Charles Ier d’Angleterre : Cat. 2
L
2indexcontenu_p_2La Tour, Maurice Quentin de : Cat. 3
3indexcontenu_p_3Léonard de Vinci : Cat. 1
P
4indexcontenu_p_4Pompadour, Jeanne Antoinette Poisson, marquise de : Cat. 3 § 3, Cat. 3 § 5, Cat. 3 § 6 et Cat. 3 § 11
R
5indexcontenu_p_5Rubens, Pierre-Paul : Cat. 2 § 3, Cat. 2 § 4, Cat. 2 § 9, Cat. 2 § 11
V
6indexcontenu_p_6Van Dyck, Antoon : Cat. 2
Catalogue
Introduction
Admirable musée du Louvre
1essai1_p_1Notre étonnement est toujours aussi grand, en parcourant notre admirable musée du Louvre, de le voir si peu fréquenté. Trop souvent le bruit des pas y résonne comme en un temple sans fidèles. Dans ce merveilleux sanctuaire d’art où, siècle par siècle, « l’idéal de tous les peuples » s’est, en quelque sorte, cristallisé en d’incomparables chefs-d’œuvre, bien rares sont les fervents qui viennent porter leur hommage et purifier leur goût. Parfois, sous la conduite d’un employé d’agence, des étrangers le parcourent et l’animent d’une rumeur passagère. Quant au Parisien, ne l’y cherchez pas : on l’y voit si peu !
2essai1_p_2Par la facilité même qu’il a d’entrer au Louvre à tout instant il remet toujours au lendemain la visite projetée. De même du provincial, venu à Paris pour ses affaires ou ses plaisirs. Il aura la plupart du temps tout vu, les promenades, les cabarets, les hippodromes, les théâtres, tout, sauf notre grand musée national.
3essai1_p_3À quoi tient cette indifférence de nos compatriotes pour les musées ? Serait-ce inaptitude à apprécier les œuvres d’art ? Je ne le pense pas, le Français ayant d’instinct le goût du Beau, d’ailleurs certifié par les merveilles d’art de notre pays. Alors ?
4essai1_p_4J’accuserais plus volontiers l’insuffisance actuelle de l’enseignement artistique dans les écoles, insuffisance qui permet à un jeune homme, d’ailleurs pourvu de parchemins, d’ignorer l’existence d’un Velázquez ou d’un Rembrandt. Que ce bon élève, un jour, pénètre dans le Louvre, il sera dès l’abord ahuri, confondu par l’entassement de ces peintures auxquelles il ne comprend rien, dont il ignore tout, l’origine, l’époque et jusqu’au nom de l’auteur.
5essai1_p_5Et ces notions élémentaires qui lui manquent, s’il lui prend fantaisie de les chercher, il ne les trouvera qu’en d’énormes volumes de critique, alourdis de considérations savantes et dont il ne pourra pas dégager la substance. Mais le guide précis, clair, facile à suivre, qui le renseignera brièvement sur la valeur d’une œuvre, la vie de son auteur, les traits essentiels de son talent, où se le procurer ? Inutile de le chercher dans les bibliothèques, il n’y existe pas. Il est encore à faire.


6essai1_p_6Ou, plutôt, il était encore à faire car, si la vanité ne nous aveugle pas, nous croyons pouvoir affirmer qu’il est fait maintenant et c’est ce guide nécessaire que nous vous présentons (Fig. 1 et Fig. 2).
7essai1_p_7La pensée directrice de cet ouvrage, c’est de propager le goût du Beau, de développer le sens artistique par la constante contemplation des plus admirables chefs-d’œuvre de la peinture. Posséder les musées chez soi, à portée de la main à toute heure, à tout instant, quelle heureuse fortune ! Le musée chez soi, c’est-à-dire évoquer la fidèle image de la toile qu’on aime, faire revivre et prolonger à son gré l’émotion ressentie devant les œuvres admirées jadis et qu’on ne reverra peut-être plus ! Quel précieux privilège de pouvoir contempler ainsi tous les tableaux célèbres, épars dans les musées les plus lointains, à Madrid, à Amsterdam, à Saint-Pétersbourg, à Rome !
8essai1_p_8Et quel concours miraculeux nous fournit la science moderne !
9essai1_p_9La photographie noire, sans lumière, uniforme de tons, a désormais vécu pour faire place à la photographie des couleurs.
10essai1_p_10Ah ! l’admirable découverte, en vérité ! Grâce à elle, la peinture nous est restituée tout entière ; c’est le tableau lui-même qui revit sous nos yeux. Regardez, tout s’y trouve, exactement rendu, le velouté des chairs, le chatoiement des étoffes, le scintillement des bijoux, la transparente légèreté des ciels, la profondeur lumineuse des ombres. Les nuances les plus fines, les frottis les moins appuyés y sont traduits avec la même précision que les plus forts empâtements. Cela n’est-il pas merveilleux, et n’est-il pas juste de dire que, possédant un tel ouvrage, on possède réellement le musée chez soi ?
11essai1_p_11Quelques lecteurs s’étonneront peut-être de rencontrer dans une sorte de désordre des œuvres très différentes d’époque, d’école et de genre. Mais cette apparente confusion n’est pas involontaire.
12essai1_p_12Elle est le résultat de considérations faciles à justifier. L’ouvrage que nous présentons au public n’est pas, en effet, purement didactique, au sens étroit du mot. Il est fait, certes, pour instruire, mais pour instruire sans ennui. Un volume d’enseignement, en matière d’art, implique généralement une classification soit par époques, soit par écoles, classification d’où se dégage toujours une certaine monotonie. Donner tout d’une traite l’école flamande, par exemple, c’est la redite obligatoire et continue des scènes d’intérieur et des scènes de cabaret, fatigantes à la longue, quelle que soit d’ailleurs la valeur intrinsèque de l’œuvre, de même que l’œil se fatiguerait aussi d’une suite ininterrompue de Madones italiennes ou de Descentes de Croix, fussent-elles signées des plus grands noms (voir Cat. 1).
13essai1_p_13Ici, au contraire, la fantaisie seule nous a guidés comme seule, dans un musée, elle guide les pas du promeneur qui s’arrête à son gré devant la toile qui l’attire, portrait, allégorie, scène d’histoire ou peinture de genre.
Une promenade pleine d’imprévu
14essai1_p_14Pareil à ce visiteur, nous n’avons prétendu faire qu’une libre promenade à travers le Louvre, promenade intéressante au plus haut point, toujours pleine d’imprévu, où chaque pas amène une surprise et une émotion nouvelles, fixant au passage les œuvres glorieuses qui rayonnent dans notre grand musée. N’est-ce point là la meilleure méthode et la plus attrayante ? Nous l’avons pensé et c’est elle que nous avons adoptée dans la présentation de ce volume.
15essai1_p_15Au hasard de la course, les époques, les écoles, les nationalités vont se confondre. L’école flamande (voir Cat. 2) voisinera souvent avec l’école française (voir Cat. 3), un Hollandais avec un Espagnol, un romantique avec un primitif, comme les fleurs les plus diverses dans un merveilleux jardin. Sans plus d’égards pour les genres, portraits (voir Cat. 1, Cat. 2, Cat. 3), allégories, sujets religieux, paysages, tableaux mythologiques alterneront au cours de ces pages, l’un nous reposant de l’autre et nous permettant de les mieux goûter tous. Ainsi conduite, la promenade est sans fatigue ; elle s’égaie de rencontres inattendues; elle puise le meilleur de son charme dans son infinie variété.
16essai1_p_16Variété qui n’enlève rien, d’ailleurs, à la portée éducative de l’ouvrage, bien au contraire, chaque planche étant accompagnée d’une notice explicative. Cette notice, nous l’avons voulue claire, précise, documentaire, débarrassée de considérations générales et dégagée des querelles d’école, assez courte pour n’être pas fatigante, assez longue pour être complète. Sur chaque œuvre reproduite elle dira tout ce qu’on en peut dire sous une forme résumée : l’événement qui en amena l’exécution, les qualités qui la distinguent, les particularités de la composition, du dessin ou du coloris, le tout fortifié par l’opinion autorisée d’un critique éminent. Du peintre lui-même nous saurons, dès le premier contact, ce qu’il importe d’en savoir, son caractère, son histoire, les anecdotes intéressantes de savie, les traits essentiels de son talent. Et lorsque le lecteur rencontrera plus loin un autre tableau du même peintre (voir Fig. 3-1), il le reconnaîtra de lui-même avant d’avoir lu le nom, sur la physionomie générale de l’œuvre, comme on reconnaît de loin un ami dans la rue avant même de distinguer les traits de son visage. Par la diversité des artistes et des œuvres, les similitudes et les différences de chacun d’eux se fixeront dans son esprit, et les classifications s’opéreront automatiquement, sans effort. Et, peu à peu, par une lente progression, sans même qu’il s’en aperçoive, il aura meublé son esprit et formé son goût. Un tel résultat suffirait à justifier cet ouvrage, ou plutôt cette série d’ouvrages, puisque, au Louvre, succéderont les Offices et le Palais Pitti de Florence, la National Gallery de Londres, l’Académie de Venise, le Prado de Madrid, les musées d’Allemagne et d’Autriche, etc.
17essai1_p_17Puissions-nous, par cette publication à la fois séduisante et éducative, avoir contribué à faire pénétrer dans le public français, d’une sensibilité artistique si grande, mais, cependant, il faut bien le reconnaître, trop souvent ignorant des merveilles qui peuplent nos musées nationaux et ceux de l’étranger, le goût de l’éternelle Beauté et le désir d’en pénétrer le mystère.
18essai1_p_18Armand Dayot
19essai1_p_19Inspecteur général des Beaux-Arts
Colophon
À propos
1colophon_p_1En publiant en ligne sa chaîne de publication d’ouvrages multiformat, le musée du Louvre poursuit son engagement vers l’accès gratuit, illimité et immédiat aux publications de la recherche scientifique. Les fonctionnalités de zoom et de manipulation des images numériques sont destinées à donner à l’édition scientifique en histoire de l’art son plein potentiel. Cet ouvrage est également disponible dans les formats ePub, PDF et en version imprimée. L’ensemble de ces formats lui garantissent maniabilité, pérennité, citabilité, référencement et présence dans les catalogues de librairies et de bibliothèques. Le musée du Louvre s’est attaché à produire un livre qui, dans tous ses formats, soit élégant et édité avec soin, afin d’offrir aux objets archéologiques et aux textes savants toute la qualité et la sensibilité attachées aux livres d’art.
Musée du Louvre
2colophon_p_2Christophe Leribault président-directeur
3colophon_p_3Kim Pham administrateur général
4colophon_p_4Francis Steinbock administrateur général adjoint
5colophon_p_5Aline François-Colin directrice des Expositions et des Éditions
Édition
colophon_h4_0Musée du Louvre
6colophon_p_6Laurence Basset directrice adjointe des Éditions
7colophon_p_7Camille Sourisse cheffe de projet, coordination et suivi éditorial
colophon_h4_1Collaborations
8colophon_p_8Nicolas Taffin C&F éditions, chef de projet, éditeur
9colophon_p_9Hervé Le Crosnier C&F éditions, suivi de projet
10colophon_p_10Julien Taquet conception et développement du site et de la chaîne de publication
11colophon_p_11Agathe Baëz conception graphique, intégration et mise en page
Informations éditeur
12colophon_p_12© musée du Louvre, Paris, 2026
13colophon_p_13https://www.louvre.fr
14colophon_p_14Ce livre est réalisé avec un assemblage d’outils libres, gratuits et open source permettant la génération de livres pour l’écran (site web) et le papier. Le site statique 11ty (https://11ty.dev). La mise en page de la version imprimée (PDF) de cet ouvrage a été réalisée avec Paged.js (https://pagedjs.org), bibliothèque javascript qui permet de transformer tout flux HTML en PDF prêt pour l’impression.
15colophon_p_15Cet ouvrage a été composé en Cooper et Basteleur.
16colophon_p_16La description des images à l’attention des personnes aveugles et malvoyantes a été réalisée par Camille Sourisse.
Obtenir cet ouvrage
17colophon_p_17Le livre est librement téléchargeable aux formats numériques ePub et PDF :
18colophon_p_18https://livres.louvre.fr/assets/louvre1912/demonstrateur.epub
https://livres.louvre.fr/assets/louvre1912/demonstrateur.pdf.
19colophon_p_19Pour une lecture optimale sur liseuse, l’ePub requiert un appareil pleinement compatible avec le format epub3.
Citer cet ouvrage
20colophon_p_20Armand Dayot (dir.), Sustainable Financing for Health. A User Guide for African Governments, Paris, musée du Louvre, 2026, https://livres.louvre.fr/louvre1912.
Foreword
1foreword_p_1For many decades, the question of how African countries can sustainably finance essential public health services has remained both urgent and complex. The continent’s development aspirations are ambitious, yet traditional financing sources have proven insufficient to meet the scale of current needs. Today, African governments simultaneously face the challenges of underfunded health systems and the escalating demands brought about by pandemics, rising incidents of non-communicable diseases, and other public health crises.
2foreword_p_2These pressures have compelled policymakers, development institutions, and financial advisors to rethink conventional approaches to public financing. The African Legal Support Facility (ALSF) recognises and supports the pressing need of governments to identify and implement tools that enable effective and sustainable health sector financing. Innovative instruments are now central to global conversations on how countries can responsibly mobilise resources while maintaining fiscal stability.
3foreword_p_3It is against this backdrop that the ALSF, with the support of the Gates Foundation, convened a diverse group of leading experts in law, finance, public health, and policy to develop “Sustainable Finance for Health: A User Guide for African Governments” (“the User Guide”). This first-of-its-kind resource responds directly to the growing interest in mechanisms such as health-focused bonds and loans, sustainability-linked debt instruments, debt-for-health swaps, and health PPPs - instruments that have been deployed globally to catalyse key investments in priority health programmes.
4foreword_p_4Despite their promise, these innovative health financing mechanisms remain underutilised, in some cases due to their legal and structural complexities. The User Guide aims to close that knowledge gap. It provides clear, practical guidance to support governments in navigating the full lifecycle of these instruments: from conceptualisation and policy alignment, to transaction structuring, documentation, negotiation, and implementation. Drawing on lessons from global initiatives such as the Global Fund to Fight Aids, tuberculosis and malaria (the “Global Fund”) and other pioneering models, it presents best practices in an accessible, actionable format.
5foreword_p_5As with previous ALSF knowledge products, this User Guide reflects the collective expertise of contributors, in this case, drawn from multilateral institutions, law firms, academia, global health organisations, and advisory practices. Their perspectives have been shaped not only by sectoral knowledge but by extensive on-the-ground experience working with and within African governments. The result is a balanced, multidisciplinary reference designed to strengthen institutional capacity across ministries of finance, health, and planning as well as among debt managers and policymakers. To ensure a collaborative and time-efficient drafting process, the User Guide was produced using the Book Sprint methodology, an intensive group writing workshop. This approach, grounded in discussion, experience sharing, and expert insight, has ensured that the final product is firmly relevant to Africa’s real-world challenges and opportunities.
6foreword_p_6We hope this User Guide will support African governments in making informed and strategic decisions as they work to scale up health sector investments and strengthen public financial management. While these materials offer guidance and practical tools, they are not a substitute for professional advice. They should be used in conjunction with tailored legal and transactional expertise - which the ALSF was established to provide and stands ready to offer.
7foreword_p_7On behalf of the African Legal Support Facility, I extend my sincere appreciation to all contributing authors, remote collaborators, facilitators, and reviewers whose dedication and expertise made this User Guide possible. I also acknowledge our partners and stakeholders across the continent, whose continued commitment to advancing sustainable financing for health consistently informs and inspires our work. In particular, I wish to express special thanks to the West African Institute for Financial and Economic Management (WAIFEM) and the Macroeconomic and Financial Management Institute of Eastern and Southern Africa (MEFMI) for their valuable support during the review process, as well as to the senior African government technical experts whose insights ensured that the User Guide reflects the practical perspectives, priorities, and collective voice of its intended end users, the African governments.
8foreword_p_8As African countries navigate a rapidly shifting global landscape, the ALSF remains steadfast in its support for solutions that promote responsible borrowing, strengthened health systems, and long-term socio-economic development. We trust that this User Guide will be a valuable resource in advancing those goals.
9foreword_p_9Olivier Pognon
Director and CEO
African Legal Support Facility
THE AFRICAN LEGAL SUPPORT FACILITY
10foreword_p_10The African Legal Support Facility (ALSF) is an international organisation which broadly aims to remove asymmetric technical capacities between public- and private-sector stakeholders. The ALSF was initially established in response to the rise in vulture fund litigation against African sovereigns, but quickly expanded to assist African governments in negotiating complex commercial transactions. The ALSF intervenes in matters related to sovereign debt, power, infrastructure and the extractive sectors.
11foreword_p_11www.alsf.org
12foreword_p_12NB: This User Guide is issued under the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International Licence (CC BY-NC-SA 4.0), which allows anyone to copy, excerpt, rework, translate and re-use the text for any non-commercial purpose without seeking permission from the authors, so long as the resulting work is also issued under a Creative Commons Licence.
A User Guide for African Governments
1homepage_p_1Sustainable Financing for Health: A User Guide for African Governments (the Guide) is a practical resource designed to support African governments in financing priority health investments in a fiscally responsible and sustainable manner. It is written primarily for Ministries of Health (MoHs) and Ministries of Finance (MoFs) and is intended to strengthen collaboration between them as they identify health priorities, assess financing options, and structure transactions that align with national development plans and macro-fiscal frameworks. The Guide responds to growing demands from governments for clear, action-focused guidance at a time of tightening fiscal space, rising debt pressures, shifting donor support, and increasing health system demands.
2homepage_p_2The Guide does not introduce new instruments. Rather, by building on established global practices and African experiences, the Guide demonstrates how existing financing mechanisms can be applied effectively to health priorities. It examines debt-for-health swaps, sustainability-linked and use-of-proceeds instruments, public-private partnerships (PPPs), and credit enhancement tools, explaining how each can be structured, governed, and implemented within national legal and institutional frameworks. Through case studies, practical tools, and structured guidance, the Guide helps officials assess readiness, manage risks, understand documentation and process requirements, and adapt these instruments to country-specific fiscal conditions and health sector needs.
Préface
1preface_p_1Lorem ipsum dolor sit amet, consectetur adipiscing elit. Nulla sed nunc enim. Vivamus eget nibh enim. Proin sed erat nulla, et pharetra massa. Ut malesuada pharetra malesuada. Aliquam at elit ut quam adipiscing accumsan. Quisque nisl lorem, adipiscing sed feugiat vel, rutrum eu arcu. Nullam aliquet metus ut lectus egestas ornare vitae quis justo. In velit odio, scelerisque sed egestas ac, cursus ac velit." Lorem ipsum dolor sit amet, consectetur adipiscing elit. Nulla sed nunc enim. Vivamus eget nibh enim. Proin sed erat nulla, et pharetra massa. Ut malesuada pharetra malesuada. Aliquam at elit ut quam adipiscing accumsan. Quisque nisl lorem, adipiscing sed feugiat vel, rutrum eu arcu. Nullam aliquet metus ut lectus egestas ornare vitae quis justo. In velit odio, scelerisque sed egestas ac, cursus ac velit." Lorem ipsum dolor sit amet, consectetur adipiscing elit. Nulla sed nunc enim. Vivamus eget nibh enim. Proin sed erat nulla, et pharetra massa. Ut malesuada pharetra malesuada. Aliquam at elit ut quam adipiscing accumsan. Quisque nisl lorem, adipiscing sed feugiat vel, rutrum eu arcu. Nullam aliquet metus ut lectus egestas ornare vitae quis justo. In velit odio, scelerisque sed egestas ac, cursus ac velit."
Executive Summary
1exec-sum_p_1Sustainable Financing for Health: A User Guide for African Governments (the Guide) is a practical resource designed to support African governments in financing priority health investments in a fiscally responsible and sustainable manner. It is written primarily for Ministries of Health (MoHs) and Ministries of Finance (MoFs) and is intended to strengthen collaboration between them as they identify health priorities, assess financing options, and structure transactions that align with national development plans and macro-fiscal frameworks. The Guide responds to growing demands from governments for clear, action-focused guidance at a time of tightening fiscal space, rising debt pressures, shifting donor support, and increasing health system demands.
2exec-sum_p_2The Guide does not introduce new instruments. Rather, by building on established global practices and African experiences, the Guide demonstrates how existing financing mechanisms can be applied effectively to health priorities. It examines debt-for-health swaps, sustainability-linked and use-of-proceeds instruments, public-private partnerships (PPPs), and credit enhancement tools, explaining how each can be structured, governed, and implemented within national legal and institutional frameworks. Through case studies, practical tools, and structured guidance, the Guide helps officials assess readiness, manage risks, understand documentation and process requirements, and adapt these instruments to country-specific fiscal conditions and health sector needs.
Why This Guide, and Why Now?
3exec-sum_p_3The timing of this Guide is critical. Many African countries are experiencing sharp reductions in Official Development Assistance, heightened debt burdens and lingering post-COVID fiscal constraints. Simultaneously, the continent faces significant population growth, persistent health service delivery gaps, and a need to increase domestic health investments. Meeting these challenges requires not just more funding but smarter financing.
4exec-sum_p_4This Guide fills an important gap in existing resources by offering an Africa-specific, government-facing tool that brings together legal, fiscal, and technical dimensions. It seeks to enhance collaboration between MoHs and MoFs, and to foster a shared understanding of what instruments are appropriate, feasible, and impactful in various circumstances.
1. Key Features
- exec-sum_ul_0
- exec-sum_li_0Modular design. The Guide is structured so that users can consult individual chapters or specific financing instruments as needed, depending on their context and role in the financing process.
- exec-sum_li_1Country ownership. Emphasises country-led planning and health sector prioritisation as the foundation for any financing solution.
- exec-sum_li_2Capacity building. Encourages institutional strengthening through embedded tools, guidance, and references complementary to ALSF and partner resources.
- exec-sum_li_3Legal clarity. Outlines the relevant legal frameworks, documentation requirements, and workflow processes required to support each instrument and related transactions.
2. Chapters
5exec-sum_p_5The Guide is designed for use by cross-functional teams of policymakers, legal experts, and technical officials working across MoHs and MoFs. It walks users through:
- exec-sum_ul_1
- exec-sum_li_4Key considerations when selecting financing instruments, including fiscal implications, regulatory requirements, and institutional capacity;
- exec-sum_li_5Practical structuring pathways and steps to design transactions that deliver tangible health impacts;
- exec-sum_li_6Decision tools to help with planning, negotiation, and implementation; and
- exec-sum_li_7Risk mitigation and governance approaches to safeguard public interest and improve execution.
6exec-sum_p_6The Guide is organised into the following nine chapters.
CHAPTER 1: SETTING THE SCENE
7exec-sum_p_7This chapter establishes the context and rationale for the Guide. It outlines the structural pressures facing African health systems, including persistent underfunding, growing disease burdens, demographic change, constrained fiscal space, and evolving donor priorities. The chapter explains why governments must move beyond reliance on traditional budgetary allocations and external aid alone, and instead take a more strategic, coordinated approach to financing health. It clarifies the purpose of the Guide as a practical tool to support MoHs and MoFs in jointly identifying, assessing, and operationalising financing solutions that are aligned with national priorities and fiscal realities.
CHAPTER 2: FINANCING FOR HEALTH
8exec-sum_p_8This chapter provides the conceptual foundation for the rest of the Guide. It explains how health financing systems function, including revenue collection, pooling of funds, and purchasing of services. It examines the different sources of health financing, domestic public expenditure, private expenditure, and external assistance, and discusses their implications for sustainability and equity. The chapter also sets out the respective and complementary roles of MoHs and MoFs, highlighting the importance of coordination between sectoral planning and macro-fiscal management. By mapping the institutional architecture and key actors involved in health financing, the chapter anchors later discussions of specific instruments within the broader system in which they must operate.
CHAPTER 3: COMMON CONSIDERATIONS
9exec-sum_p_9Chapter 3 focuses on the cross-cutting conditions that must be in place for financing instruments to be effective and sustainable. It highlights the legal, regulatory, and institutional frameworks that shape health financing decisions, including public financial management systems, debt management rules, procurement frameworks, and approval processes. The chapter underscores the importance of regulatory alignment, fiscal risk assessment, transparency, and inter-ministerial coordination. It also addresses institutional capacity, governance arrangements, and the need to tailor financing solutions to country-specific legal and fiscal contexts. This chapter serves as a readiness lens, helping officials assess whether the enabling environment can support the instrument under consideration.
CHAPTER 4: HEALTH FINANCE AND KEY PERFORMANCE INDICATORS
10exec-sum_p_10Chapter 4 links financing to outcomes. It begins by situating national health financing within the broader global health architecture, including the role of major international institutions and financing partners that support health investments across Africa. It then outlines the main categories of health expenditure and typical programmatic areas financed within the sector. The central focus of the chapter is the role of key performance indicators (KPIs). It explains how measurable indicators are used to connect financing to results, particularly in performance-based, sustainability-linked, and results-oriented instruments. By clarifying how KPIs are defined, monitored, and verified, the chapter provides the analytical bridge between financial structuring and measurable improvements in health outcomes.
CHAPTER 5: SUSTAINABLE FINANCE INSTRUMENTS
11exec-sum_p_11Chapter 5 aims to guide officials from MoFs and MoHs, as well as practitioners, on the design and implementation of sustainable financing instruments - specifically use of proceed and sustainability-linked bonds and loans, and impact bonds as mechanisms to mobilise public and private capital for health objectives. It explains core structuring elements, including the identification of eligible health expenditures or measurable KPIs and sustainability performance targets, and highlights the importance of credible monitoring, reporting, and verification systems aligned with market standards.
12exec-sum_p_12The chapter also addresses the supporting legal and transactional frameworks for such instruments, including the preparation of sustainable finance frameworks, external reviews, and the incorporation of binding use of proceeds, reporting, and performance related provisions in bond or loan documentation. It sets out enabling conditions, inter-ministerial coordination requirements, and includes practical checklists and workflow processes to guide governments from preparation through issuance and ongoing compliance.
CHAPTER 6: DEBT-FOR-HEALTH SWAPS
13exec-sum_p_13This chapter explains the structure and rationale of debt-for-health swaps, under which a portion of external debt is cancelled, reduced, or restructured in exchange for a commitment to invest agreed amounts in priority health programmes. The chapter distinguishes between bilateral debt swaps, concluded between official bilateral creditors and debtor governments, and commercial debt conversions involving private creditors, often supported by intermediaries or credit enhancers. The chapter outlines the potential benefits, including fiscal space creation and targeted investment in health, as well as key risks such as complex negotiations, governance and fiduciary challenges, and possible implications for credit ratings and future market access.
14exec-sum_p_14In addition, the chapter sets out the transaction architecture and process steps required to operationalise a swap. It describes the preparatory phase, including debt stock analysis, identification of eligible obligations, stakeholder mapping, and alignment with national health priorities. It outlines the negotiation and structuring phase, including term sheet development, creditor engagement, and the design of governance and oversight arrangements for the health investment component.
15exec-sum_p_15Finally, the chapter highlights the legal documentation typically required, such as framework agreements, swap agreements, trust or fund arrangements, and implementation protocols, as well as monitoring and reporting mechanisms to ensure transparency, accountability, and measurable health outcomes. Practical process maps and checklists are provided to guide ministries through feasibility assessment, negotiation, documentation, and post swap implementation.
CHAPTER 7: THE USE OF PUBLIC-PRIVATE PARTNERSHIPS IN HEALTHCARE PROJECTS
16exec-sum_p_16Chapter 7 provides structured guidance on the application of PPPs in the health sector. Part 1 of this chapter clarifies the defining features of health PPPs, the policy objectives they can serve, and the circumstances in which they are suitable. It emphasises value for money, fiscal affordability, risk allocation discipline, and the need to align PPP structures with national health priorities and public financial management frameworks.
17exec-sum_p_17Part 2 sets out the full PPP lifecycle, from project identification and screening through feasibility analysis, structuring, procurement, contract award, and long-term contract management. The chapter includes practical tools such as project screening criteria, feasibility and affordability assessment guidance, risk allocation matrices, procurement integrity safeguards, and contract management checklists. It also highlights the key legal considerations underpinning health PPPs, including enabling legislation, procurement compliance, contractual documentation, performance and payment mechanisms, dispute resolution provisions, and ongoing monitoring and reporting obligations. Together, these tools and process maps are intended to guide officials in structuring bankable, transparent, and accountable health PPP transactions.
CHAPTER 8: CREDIT ENHANCEMENT
18exec-sum_p_18Chapter 8 explains how credit enhancement can improve access to finance for health by reducing perceived risk and lowering the cost of capital. It sets out the main credit enhancement options used in practice, including partial and full guarantees, political risk insurance, liquidity facilities, reserve accounts and cash collateral structures, and other forms of risk sharing with development finance institutions and insurers. The chapter guides officials on how to select an appropriate instrument based on the underlying transaction, the risk being addressed, and the intended impact on pricing, tenor, and investor appetite.
19exec-sum_p_19The chapter also provides practical guidance on structuring and implementation. It outlines key questions for assessing feasibility, including the trigger conditions, coverage scope, claims process, and interaction with the base bond or loan terms. It highlights the main legal and governance considerations, including authority to issue or accept guarantees, approval and procurement requirements, disclosure and reporting obligations, and recording contingent liabilities in line with public debt and fiscal risk management frameworks.
CHAPTER 9: RECOMMENDATIONS
20exec-sum_p_20The final chapter provides recommendations aimed at strengthening the enabling environment for health financing transactions and improving decision-making. It separates recommendations for MoHs and MoFs, focusing on planning, cross government collaboration, realistic budgeting, and stronger risk and contingent liability management.
Key recommendations at a glance
21exec-sum_p_21Recommendations for MoHs include:
- exec-sum_ul_2
- exec-sum_li_8Advocate for fair and realistic allocations to health.
- exec-sum_li_9Take a long-term, strategic view in financing health priorities.
- exec-sum_li_10Build credible execution capacity and data-driven delivery.
- exec-sum_li_11Collaborate closely with the MoF to design and execute health financing instruments.
22exec-sum_p_22Recommendations for MoFs include:
- exec-sum_ul_3
- exec-sum_li_12Put blended finance tools at the centre of national borrowing plans.
- exec-sum_li_13Ensure visibility over budget execution for the health sector.
- exec-sum_li_14Standardise and improve health finance data.
- exec-sum_li_15Establish a task force to mobilise credit enhancement for health funding.
- exec-sum_li_16Build the capacity of the MoF and the MoH to jointly engage in innovative financing instruments.
23exec-sum_p_23Overall, the Guide supports governments to make better structured choices, grounded in law, public finance rules, and implementation capacity. It encourages early collaboration between health and finance teams, careful use of indicators and safeguards, and disciplined use of advisors and documentation so that financing decisions translate into deliverable health outcomes.
Contributing Authors
Chapter 1: Setting the Scene
1chap1_p_1Health is central to sustainable development. Across Africa, governments face the dual challenge of improving health outcomes and access to healthcare while preserving fiscal sustainability. Historically, African countries have relied heavily on Official Development Assistance (ODA) to finance their health objectives, with ODA accounting for 30-50% of Total Health Expenditure (THE) in low-income settings. Yet, global aid is contracting and health support is declining even faster, reaching its lowest level in over a decade.
2chap1_p_2This comes at a time when public health emergencies are on the rise (a report by Africa CDC: Africa’s Health Financing in a New Era - April 2025, reports a 41% increase, from 152 in 2022 to 213 in 2024), exposing chronic underinvestment in health infrastructure and in healthcare workers (HCWs). The COVID-19 pandemic highlighted that health is not only a social priority but also a foundation of economic resilience and national security. Meanwhile, global health institutions such as the World Health Organisation (WHO), the Global Fund to Fight Aids, tuberculosis and malaria (Global Fund), Gavi and the World Bank continue to play a pivotal role in financing and technical assistance. Still, their focus is shifting toward catalytic funding models (a type of financing that seeks to create positive social and environmental impacts in addition to generating financial returns), co-financing requirements and greater country ownership, underscoring the need for governments to mobilise sustainable domestic resources and to leverage innovative financing instruments.
Objectives of the User Guide
3chap1_p_3This User Guide is a practical, action-oriented resource for African governments, particularly for ministries of health and finance, on designing, negotiating and implementing sustainable health financing solutions - in particular sustainable financing instruments, debt swaps and public-private partnerships. It simplifies these complex tools and provides clear frameworks for assessing readiness, structuring transactions and ensuring long-term value for health systems. While the Ministry of Finance (MoF) leads on fiscal and debt-related engagements, the Ministry of Health plays a critical role in defining the investment case, aligning interventions with national priorities and ensuring that the proceeds of innovative financing directly strengthen health outcomes and systems. The User Guide promotes a shared understanding of how finance and health authorities can collaborate to leverage financial innovation for tangible benefits to population health and resilience.
Note on One Health and Cross-Sectoral Collaboration4chap1_p_4Throughout this Guide, references to the “Ministry of Health” should be understood in a broader context that aligns with the One Health approach. In many countries, the health sector includes several line ministries and government agencies working across human, animal, and environmental health. While the Ministry of Health is typically the lead actor, successful health financing strategies often require coordination with other relevant ministries, including those responsible for agriculture, environment, social protection, and infrastructure. This Guide encourages governments to adopt inclusive approaches that reflect their national institutional arrangements and health priorities. 5chap1_p_5For more details on the One Health approach and its implications for health financing and cross-sectoral coordination, the reader is referred to the World Health Organization (WHO), Food and Agriculture Organization (FAO), and World Organisation for Animal Health (WOAH) joint One Health framework, which highlights the interdependence of human, animal, and environmental health sectors and the importance of integrated planning and resource mobilisation at https://www.who.int/health-topics/one-health |
How the User Guide Complements Existing Tools
6chap1_p_6While several frameworks and publications exist on health financing, this User Guide provides an African-led perspective on health systems and their funding challenges. It also suggests frameworks for undertaking transactions with deliverable financing instruments that are grounded in legal and institutional realities. It builds on existing strategies and tools by bridging the gap between planning and execution, offering practical guidance on additional options for revenue mobilisation, deal structuring and legal considerations. It complements national health financing strategies, expenditure frameworks and toolkits developed by the WHO, Gavi, the Global Fund and other partners.
How to Use It
7chap1_p_7Rather than being read from cover to cover, the User Guide is organised in a modular format. Users can engage with specific instruments or tools based on their needs, stage of the financing process or institutional role. The resource can be used in several ways:
- chap1_ul_0
- chap1_li_0As a capacity-building tool, it aims to deepen understanding of instruments like thematic and sustainability-linked bonds, debt-for-health swaps and health-related public-private partnerships (PPPs).
- chap1_li_1As a readiness assessment tool, it guides policymakers in understanding and evaluating the enabling conditions, fiscal space and institutional preparedness required to obtain such financing.
- chap1_li_2As a legal and negotiation reference, with model clauses and checklists to support transaction teams.
- chap1_li_3As a decision-support guide, it helps policymakers assess the appropriateness of different instruments in light of fiscal realities and health priorities.
- chap1_li_4As a coordination guide, supporting joint planning between MoHs and MoFs, other government departments and agencies and other stakeholders.
8chap1_p_8Throughout, the User Guide draws on real-world examples. Importantly, however, it is intended to complement, not replace, national policies, legal frameworks or planning processes.
9chap1_p_9Users are also encouraged to consult related resources such as the ALSF Sovereign Debt Handbook and ALSF Debt Document Commentaries for technical insights into legal structuring and compliance, in particular, the ALSF Sustainability Financing Debt Guide and the ALSF Debt Swaps Guide.
What This User Guide Is Not
10chap1_p_10While this User Guide provides a robust foundation for understanding and applying health financing instruments, it does not purport to contain all the information each user may require on such instruments. It is also not a substitute for professional legal, financial or technical advice. The design and execution of complex transactions, especially those involving PPPs or sovereign borrowing, require the expertise of qualified professionals. Governments are strongly encouraged to seek such support in all phases of implementation.
Chapter 2: Financing for Health
1chap2_p_1This chapter provides the background and rationale for the User Guide. It explains why health is central to sustainable development, outlines the current financing challenges related to health systems in African countries and introduces the key financing instruments outlined in the resource. It also begins to identify everyday health expenditures and indicators that lend themselves well to these external financing options, as well as key considerations that governments must take into account when choosing the indicators.
Why Health Matters
2chap2_p_2Health is both a moral imperative and a foundation for economic and social development. The global community’s commitment to health is enshrined in the Sustainable Development Goals (SDGs), particularly SDG 2 (Zero Hunger) and SDG 3 (Good Health and Well-being). These set ambitious goals to substantially and sustainably improve the health of all people. Yet, beyond moral obligation, the case for investing in health is also profoundly economic. Healthier populations are more productive, more resilient and more capable of driving long-term national growth.
3chap2_p_3Evidence from across regions shows that investments in health yield among the highest returns of any public expenditure. Global analyses from the World Health Organisation (WHO) and the Global Fund suggest an average return on investment exceeding 30:1. These gains reflect the multiple channels through which health fuels development, from reducing absenteeism and increasing labour productivity to enhancing children’s learning outcomes and enabling women’s greater participation in the workforce.
4chap2_p_4Most importantly, health remains one of the issues citizens care about the most. The 2024 Afrobarometer survey found that health ranks second, on average, among the most critical problems for governments to address, behind only unemployment. This demand reflects a simple reality: when people are healthy, communities thrive, economies function and social contracts are strengthened.
5chap2_p_5For policymakers, therefore, investing in health is not just about meeting humanitarian goals; it is about safeguarding the very foundations of growth and stability. Recognising this link between health and prosperity is essential for both Ministries of Health (MoHs) and Ministries of Finance (MOFs) as they navigate the choices and trade-offs that shape national development.
The Funding Crisis
6chap2_p_6Over the past two decades, Africa has made remarkable gains in health: access to care has expanded, maternal and child mortality have fallen, and coverage of key services, such as immunisation, human immunodeficiency virus (HIV) treatment and other disease programmes, has increased significantly. These achievements reflect the dedication of governments, communities and development partners working to strengthen health systems and broaden service reach.
7chap2_p_7Much of this progress has been underpinned by external financing. For years, organisations such as the Global Fund, Gavi, the World Bank and significant bilateral donors have provided the resources that have helped to close domestic funding gaps.
8chap2_p_8That financial landscape is now changing rapidly. In 2024, total Official Development Assistance (ODA) from the Organisation for Economic Co-operation and Development - Development Assistance Committee members declined by 7.1% in real terms. In 2025, countries in sub-Saharan Africa are expected to see a 16-28% reduction compared to 2021, the most significant reduction among all regions. Additionally, health-specific aid is declining at a faster rate than other sectors. The most prominent donors, accounting for 80% of bilateral health and population aid, are expected to reduce their ODA contributions, with the United States alone providing over half of the historical contributions. These contractions occur at a time when health systems are under increasing pressure, as evidenced by the 41% increase in public health emergencies between 2022 and 2024.OECD. (n.d.). Official development assistance (ODA). Organisation for Economic Co-operation and Development. https://www.oecd.org/en/topics/policy-issues/official-development-assistance-oda.html
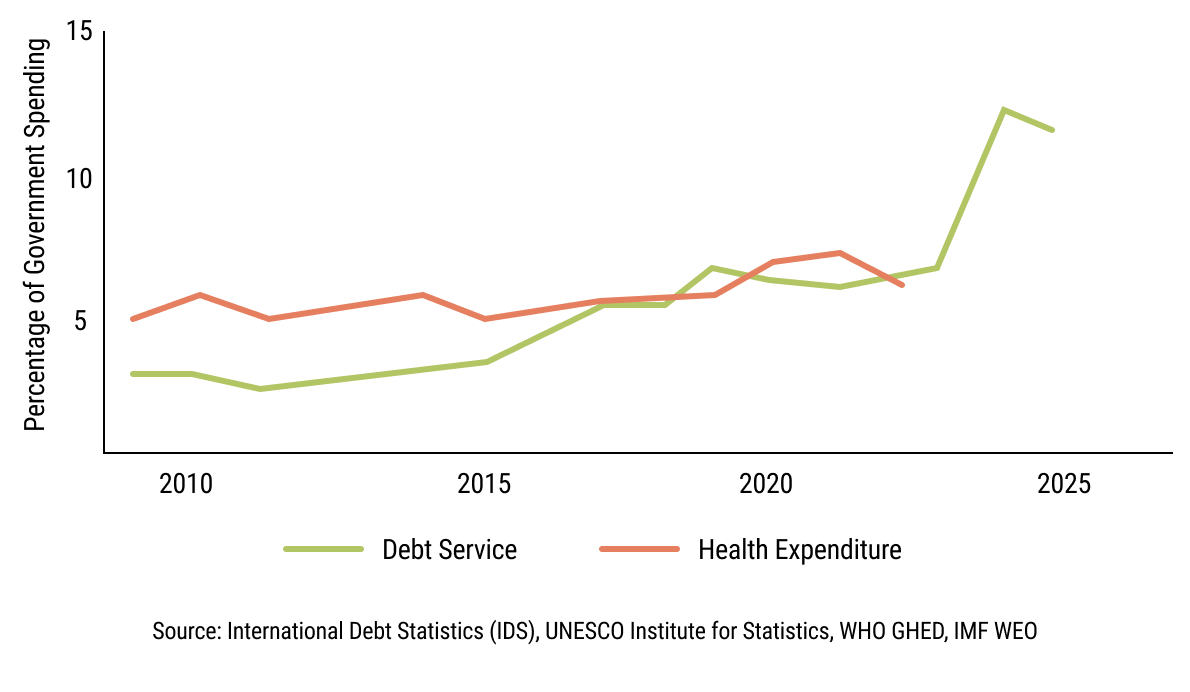
9chap2_p_9The decline in donor funding is exacerbated by a dramatically tightening fiscal space within African governments. At least 22 countries on the continent are now in or at high risk of debt distress, and more than 30 countries pay more annually on debt servicing (the total amount of money required to pay the interest and principal on existing debt) than on their health sectors.
 chap2_img_0
chap2_img_010chap2_p_10This triple pressure - shrinking external support, increasing healthcare needs and increasing debt servicing on existing debt obligations - forces governments to balance the imperative of improving health outcomes with the need to preserve macroeconomic fiscal stability. The result is a growing mismatch between what citizens need and what national budgets can sustainably deliver.
11chap2_p_11This is where collaboration between MoHs and MoFs becomes essential. Together, they must look beyond traditional budget allocations to identify and implement financing instruments, such as public-private partnerships (PPPs), debt swaps and other sustainable debt instruments that can expand fiscal space for health while maintaining financial sustainability. They should also consider the shifting roles of major health funders, such as the Global Fund, Gavi and the World Bank, as described in Chapter 4: Health Finance and Key Performance Indicators.
Case Study: Situating This User Guide Within National Health Financing Strategies12chap2_p_12Every country’s path to universal health coverage (UHC) is unique, but the principles of sound health financing remain the same. Health financing strategies are designed to chart a financially feasible pathway toward UHC, ensuring that everyone can access the health services they need without suffering financial hardship. Progress is measured along three dimensions: the range of services provided, the share of the population covered and the extent to which individuals are protected from out-of-pocket costs. 13chap2_p_13Within this broader framework, this User Guide offers practical options for governments seeking to increase health expenditure and move closer to UHC sustainably. It focuses on three financing instruments - PPPs, debt swaps and sustainable debt instruments - that can help countries mobilise and channel additional resources for health. However, these options are not stand-alone solutions. They should be considered complementary tools that operate within and are guided by a country’s overarching health financing strategy. 14chap2_p_14As the WHO Health Financing Guide explains, effective financing systems rely on three interconnected functions:
15chap2_p_15The instruments discussed in this User Guide primarily strengthen the first of these functions - resource mobilisation - while also linking to aspects of strategic purchasing, particularly through the PPP approach and impact bonds. 16chap2_p_16It is important to emphasise that this User Guide is not a substitute for a comprehensive health financing strategy. MoHs should continue to lead on developing and updating such strategies as a roadmap toward UHC - setting priorities, defining service packages and identifying reforms that improve efficiency and effectiveness. This includes maximising the impact of existing budgets through better prioritisation, stronger budget execution and more effective provider payment mechanisms. 17chap2_p_17Ultimately, the guidance provided here is intended to complement those broader efforts - equipping MoHs and MoFs with the tools, language and frameworks needed to explore new financing opportunities, while maintaining alignment with national health goals and fiscal sustainability. |
Proposed Solutions
Overview of Financing Structures
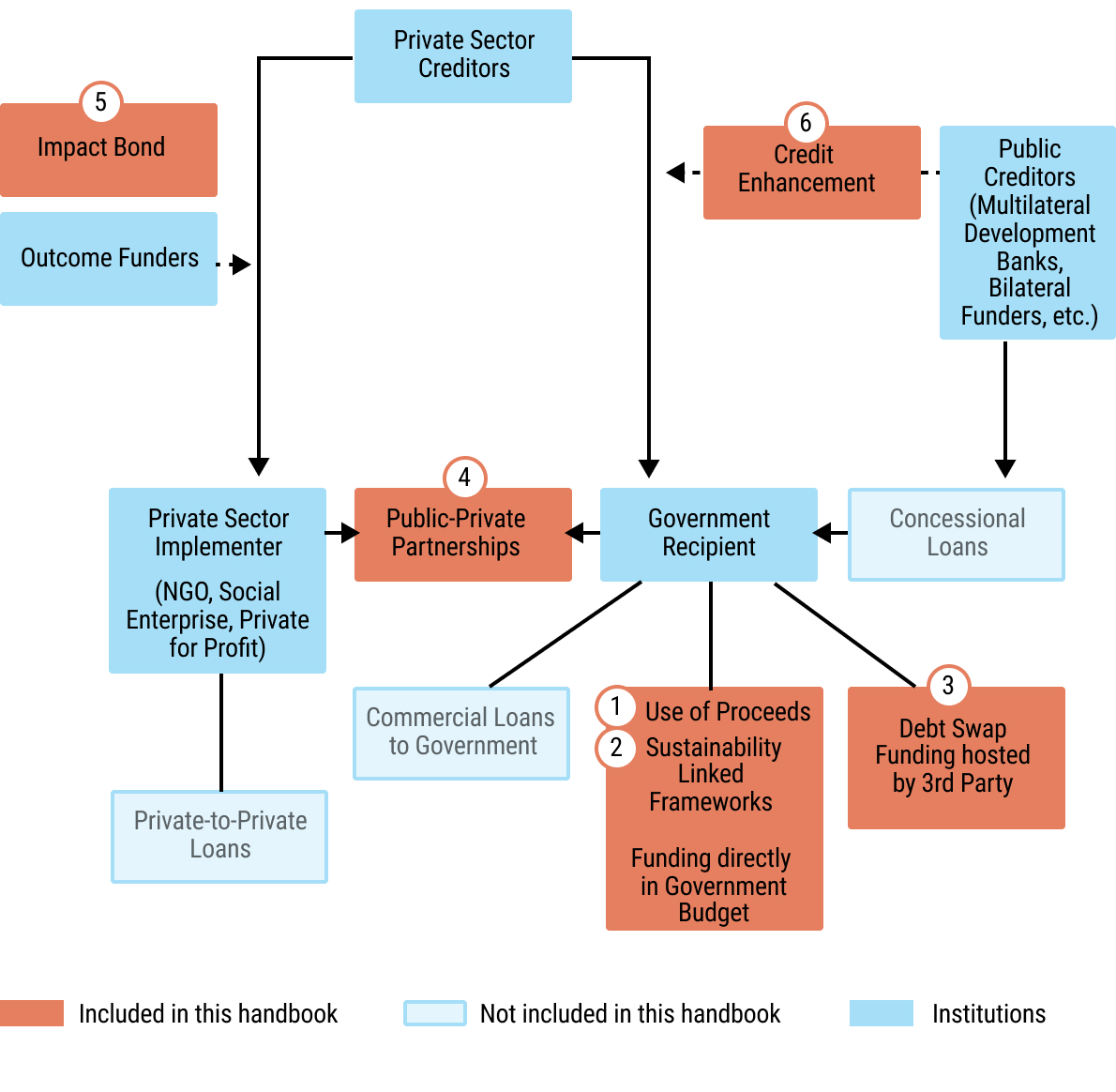
18chap2_p_18Several potential solutions exist for filling the financing gap that can be used simultaneously. This User Guide focuses on three categories of instruments, some of which have been rarely used in the health sector. However, they provide promising new opportunities for additional funding in the health sector. The User Guide does not address private funding that is channelled towards private sector implementers, but instead focuses on raising funds for the public sector. These instruments have been prioritised based on the African Legal Support Facility’s (ALSF) experience in responding to country requests for technical assistance in exploring and implementing them.
 chap2_img_1
chap2_img_1
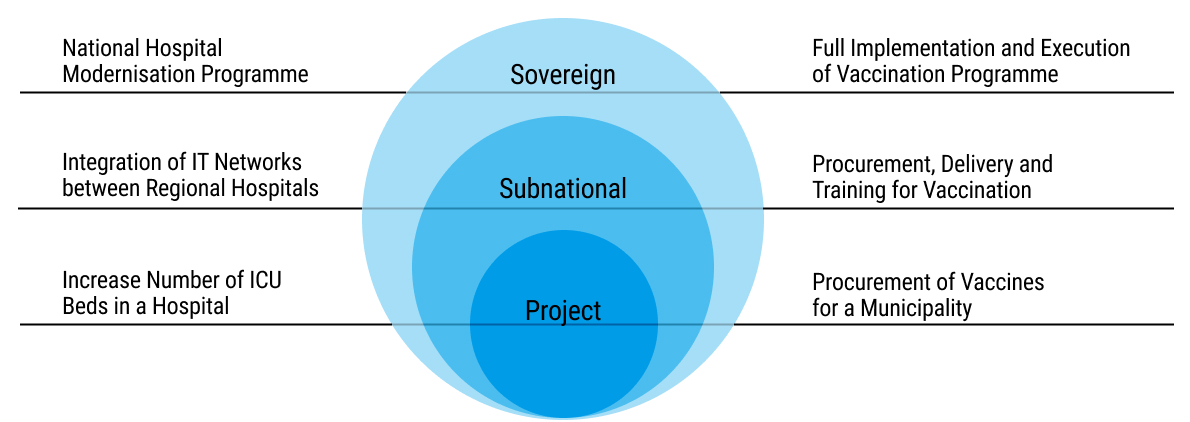
19chap2_p_19These instruments can be applied across different levels: the sovereign level (I.e. national level), sub-sovereign level (I.e. state or county level) or based on a specific project:
20chap2_p_20
 chap2_img_2
chap2_img_2
Financing Instruments
21chap2_p_21Some of the financing solutions discussed in this User Guide are novel to the health sector but have already been successfully used in other sectors. For instance, sustainable financing solutions often include those focused on deforestation or renewable energy, as well as debt swaps for marine conservation or education. PPPs, in contrast, have been in use in the health sector since the 1980s but have received more attention recently.
22chap2_p_22This User Guide outlines the following instruments:
Use of Proceeds Bonds or Loans
23chap2_p_23A use of proceeds loan or bond ties financing to specific projects and expenses (see Chapter 5: Sustainable Finance Instruments for a detailed description of use of proceeds loans and bonds).
24chap2_p_24Such instruments typically follow market best practices (e.g. relevant International Capital Market Association (ICMA) and Loan Market Association (LMA) Principles), as described in Chapter 4: Health Finance and Key Performance Indicators, as well as Chapter 5: Sustainable Finance Instruments.
Sustainability-Linked Financing (SLF): Sustainability-Linked Loans (SLL) And Sustainability-Linked Bonds (SLB)
25chap2_p_25An SLF is new funding, such as a loan or a bond, that is tied to specific Key Performance Indicators (KPIs), which are the basis for setting Sustainability Performance Targets (SPTs). The proceeds from the SLF will be allocated to the general budget.
26chap2_p_26The key component of an SLF, as opposed to a plain loan or bond (the distinction between loans and bonds is described in more detail in Chapter 5: Sustainable Finance Instruments), is that the investor is interested in the country achieving agreed performance metrics. Accordingly, the level of interest payments on the instrument will increase or decrease depending on whether the SPTs are met. For example, the SLF may outline a Human Immunodeficiency Virus (HIV) prevention performance target to be achieved within 5 years. Regular monitoring will be necessary for the performance metrics, and the country may be incentivised or penalised for over- or underachieving against these targets.
27chap2_p_27Such instruments are structured in accordance with market best practices (e.g. relevant ICMA and LMA Principles), as described in Chapter 5: Sustainable Finance Instruments.
Impact Bonds
28chap2_p_28An impact bond is a results-based financing arrangement between a government or grant funder, an investor and a service provider. The investor provides upfront funding for service delivery, and the funder only pays if pre-agreed health outcomes are achieved. Although named as a “bond”, it is not a tradable instrument; rather, it is a private investment where returns depend entirely on whether the agreed-upon outcomes are met. Impact bonds are typically small in size, usually under USD 10 million.
Debt Swaps
29chap2_p_29A debt swap is when part of a country’s debt is cancelled or replaced with cheaper debt, and the government agrees to use some, or all, of the money it saves to fund specific priority programmes. In effect, the transaction creates fiscal savings that are allocated to health expenditures. Debt swaps enable governments to earmark regular, predictable government spending over a long period, and are well-suited for funding long-term health priorities.
30chap2_p_30Two forms of debt swaps are covered in this User Guide:
- chap2_ol_1
- chap2_li_3Bilateral debt swaps. A bilateral debt swap is an agreement between a debtor country and a creditor government to cancel or convert part of the debt owed in exchange for the debtor investing an equivalent amount in agreed national projects or programmes.
- chap2_li_4Commercial debt conversions. This occurs when private sector debt is replaced with a new instrument (e.g. a new loan) under more favourable terms. Some or all of the money saved through the lower interest rate (obtained through the involvement of a credit support provider) and potentially a debt reduction is then contractually obligated to be utilised on specific spending or outcomes.
Public-Private Partnerships
31chap2_p_31A PPP is a mechanism that mobilises private funding for delivering public infrastructure and/or services. Blending commercial funding with government grants and/or concessional loans helps improve the financial viability of PPPs where projects are economically or socially essential but not commercially attractive enough for private investors.
32chap2_p_32Financing may come entirely from public sources, such as national programmes to control infectious diseases, from private sources, such as out-of-pocket expenditure for elective procedures or dentistry and from a mix of both, such as public insurance that pays for services delivered by private providers.
|
33chap2_p_33Instrument |
34chap2_p_34Primary Objective |
35chap2_p_35Typical Scale |
36chap2_p_36Relevance to Health |
37chap2_p_37Chapter |
|
38chap2_p_38Health Bonds & Loans |
39chap2_p_39The borrowed amount has to be spent on equivalent health-related expenditures |
40chap2_p_40Medium - Large |
41chap2_p_41Incentivise the increase in the health budget |
42chap2_p_42Chapter 4: Health Finance and Key Performance Indicators |
|
43chap2_p_43SLFs |
44chap2_p_44Tie borrowing costs to measurable health outcomes |
45chap2_p_45Medium - Large |
46chap2_p_46Incentivise performance and accountability |
47chap2_p_47Chapter 4: Health Finance and Key Performance Indicators |
|
48chap2_p_48Impact Bonds |
49chap2_p_49Combine public and private funds to achieve pre-agreed outcome targets delivered by a service provider |
50chap2_p_50Small |
51chap2_p_51Incentivise the performance of a non-governmental implementer |
52chap2_p_52Chapter 4: Health Finance and Key Performance Indicators |
|
53chap2_p_53Debt Swaps |
54chap2_p_54Convert significant amounts of debt repayments into health investments |
55chap2_p_55Small - Medium |
56chap2_p_56Free up fiscal space for priority programmes |
57chap2_p_57Chapter 6: Debt-for-Health Swaps |
|
58chap2_p_58PPPs |
59chap2_p_59Mobilise private investment in health infrastructure/services |
60chap2_p_60Large |
61chap2_p_61Expand capacity sustainably |
62chap2_p_62Chapter 7: The Use of Public-Private Partnerships in Healthcare Projects |
Key Considerations in Selecting Instruments and Health Priorities
63chap2_p_63There are three common considerations when selecting the type of instrument to use:
Scale of Funding
64chap2_p_64Both MoHs and MoFs are interested in how much funding can be mobilised to support health or the general budget. When considering the instruments, how much money is mobilised will be a key consideration.
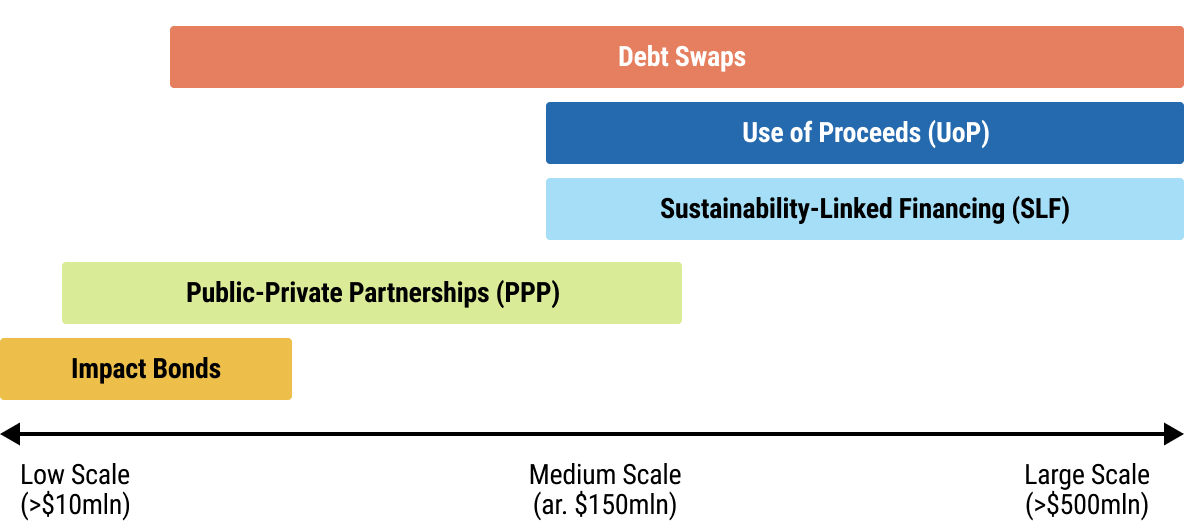 chap2_img_3
chap2_img_3
Fig. 2.4: Financing Instruments
Indebtedness
65chap2_p_65In addition to considering the amount of debt raised, MoFs need to consider the country’s debt-carrying capacity (I.e. the maximum level of debt a country can sustainably incur and service without entering into financial distress). When debt levels are low, instruments such as health bonds and SLFs may be suitable as they allow governments to raise capital for sustainable development. For countries with high but still manageable debt, PPPs can be appropriate, as they mobilise private and/or concessional capital without significantly adding to public debt burdens. Note that SLFs can also help improve debt sustainability by refinancing or buying back outstanding debt.
66chap2_p_66Debt swaps can be helpful by way of liquidity support, as they offer a tailored and effective way to lower debt servicing costs and in some instances also the debt to GDP ratio of the country (especially where any publicly traded bonds repurchased as part of the debt conversion are trading at high discounts) and channel fiscal savings into health-related programmes which would otherwise be unfunded.
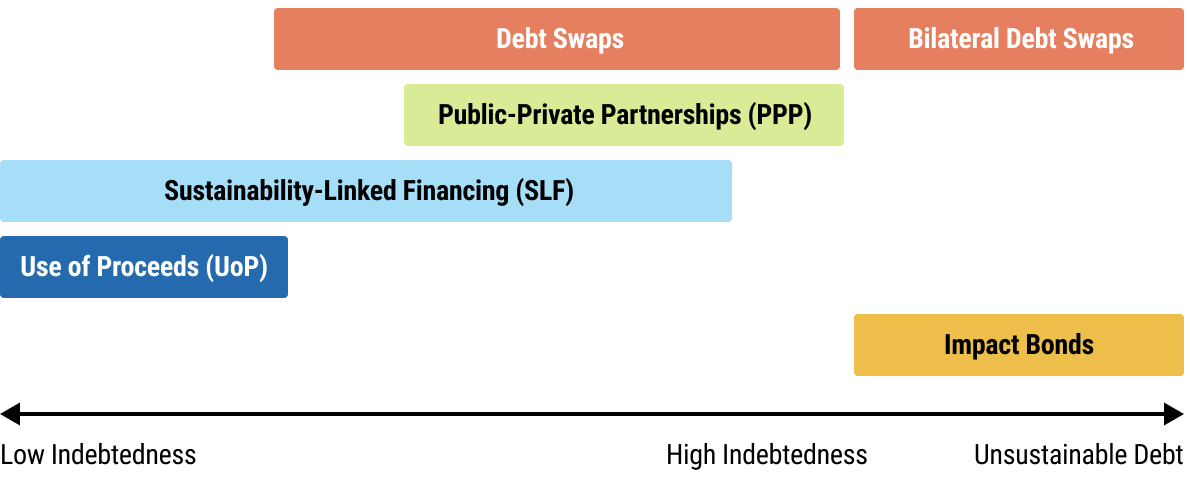 chap2_img_4
chap2_img_4
Specificity
67chap2_p_67Financing instruments differ in the extent to which the funds raised must be used for specific purposes. In some cases, such as health loans, bonds and impact bonds, the funding is tied to specific activities or outcomes. Other instruments, such as SLLs and SLBs, are included in the general budget, allowing for significant flexibility in spending decisions during the implementation phase.
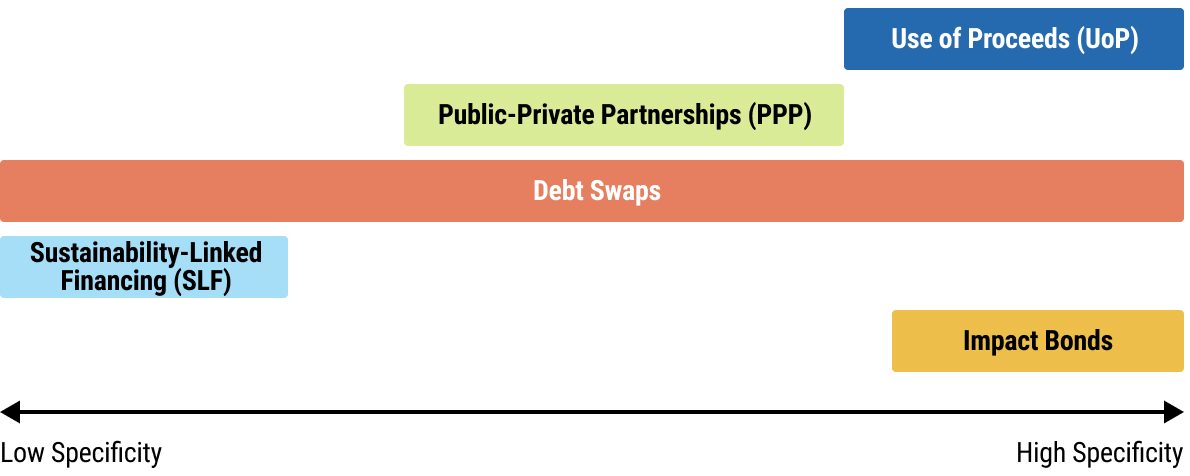 chap2_img_5
chap2_img_5
Chapter 3: Common Considerations
1chap3_p_1This chapter outlines a set of common considerations that underpin the effectiveness of the various financing instruments for health presented in this User Guide, including sustainability-linked financing (SLF), debt swaps and public-private partnerships (PPPs). Each component is based on international best practices and shaped by lessons from country experiences.
2chap3_p_2For Ministries of Health (MoHs), this chapter explains how to maximise the sectoral impact of financing by identifying priority interventions, strengthening reporting and monitoring systems and ensuring that health results remain central throughout the design process. For Ministries of Finance (MoFs), it emphasises the importance of fiscal prudence, debt sustainability and coherent integration into macroeconomic frameworks. Both institutions share the responsibility of ensuring that any innovative instrument aligns with the country’s institutional capacity, legal frameworks, debt-carrying capacity and broader development strategy.
3chap3_p_3Ultimately, success in health financing innovation depends on collaboration. The design of these instruments must build on, not bypass, national systems and processes. They work best when treated as an extension of sound governance and coordinated reform, not as isolated financial products.
4chap3_p_4By the end of this chapter, readers will understand the common factors that determine whether non-traditional and structured financing instruments, such as SLFs, debt swaps and PPPs, can achieve meaningful and lasting results in a particular country context. Success depends not only on financial design but also on how each mechanism strengthens national systems, aligns with fiscal and health priorities and fosters institutional learning.
Prioritising Health Financing Impact
5chap3_p_5Financing instruments are most effective when financial innovation is matched with strategic alignment. The goal is not simply to mobilise new resources for health, but also to ensure that all funds raised deliver measurable and lasting results. This requires clear linkage to national health strategies, well-defined activities and realistic assessments of financing needs and absorptive capacity.
6chap3_p_6Every transaction should begin with clarity on the health priorities it will support and how the proceeds will be used. These priorities must be anchored in existing national plans or sectoral strategies, transparently costed and matched with a financing mechanism suited to their scale, purpose and timeline.
7chap3_p_7Governments also need credible data and reporting systems to meet the accountability standards tied to these instruments. Where national data systems are still maturing, temporary reliance on established global or regional platforms may be appropriate, but should be paired with efforts to build domestic capacity for tracking both financial and health outcomes. Over time, this ensures that financing arrangements strengthen country systems rather than create parallel ones.
8chap3_p_8For sustainability-linked financing, the careful selection of key performance indicators (KPIs) is essential. Indicators must be measurable, meaningful and achievable - ambitious enough to drive results, but realistic enough to be credible. Well-designed KPIs enhance confidence and attract further investment; weak or superficial ones erode both confidence and investment.
9chap3_p_9The MoH has a vital advocacy role in securing an appropriate share of funds for health within debt or SLF arrangements. Together, MoHs and MoFs must assess the full cost of each mechanism, including the overall costs and expenses of the transaction at inception (including advisory, legal and third-party fees), ongoing costs and expenses and debt servicing costs, to ensure that the net fiscal and health benefits justify the investment.
10chap3_p_10Ultimately, the measure of success is not the volume of financing mobilised, but whether the application of such funding strengthens, sustains and makes health systems more equitable and resilient over time.
11chap3_p_11For more detailed information on KPIs and health systems, see Chapter 4: Health Finance and Key Performance Indicators.
Managing the Fiscal and Debt Implications of Financial Instruments
12chap3_p_12Before considering sustainability-linked or health-related financing, debt management offices (DMOs) must first ensure these instruments fit within the annual borrowing plan defined in the national budget and align with the national Medium-Term Debt Strategy (MTDS). Indeed, potential instruments need to be assessed against the country’s financing needs as well as its debt management objectives, including impact on refinancing risk, interest rate risk and foreign currency risks.
13chap3_p_13DMOs also need to assess, ex ante, the overall impact of the financing instrument on public debt sustainability in the context of the country’s debt carrying capacity. This will often involve modelling debt sustainability analysis (DSA) scenarios reflecting the target structure of the contemplated instruments. This analysis will inform the range of acceptable terms, including the total amount of funding to be raised, acceptable interest rates (and, in this context, whether third-party credit support would be beneficial) and repayment periods. For PPPs, a contingent liability risk assessment enables the safeguarding of longer-term fiscal and debt sustainability.
14chap3_p_14Exploring credit-enhancement mechanisms will be crucial to improving terms and reducing funding costs for borrowers. However, as these solutions often come with additional expenses, such as guarantee or insurance premiums, performing a comprehensive cost assessment is essential to determine whether the participation of credit enhancement providers lowers the overall costs of funding (see also Chapter 8: Credit Enhancement). In some cases, philanthropic or concessional capital can be mobilised to cover these premiums, partially or entirely. In the case of loan-based financing, running a competitive and transparent selection process among several international lenders can also help optimise pricing and terms.
15chap3_p_15While these instruments generally signal a strong commitment to macroeconomic fiscal sustainability, governments must remain alert to potential credit perception risks. For instance, some commercial debt swaps could be classified by rating agencies as distressed exchanges, where low-rated countries buyback bonds in the capital markets as part of a debt swap under liquidity stress. Early engagement and transparent communication with rating agencies is therefore essential to understand the rating methodologies of the respective rating agencies and their implications for the proposed debt swap.
16chap3_p_16Finally, countries need to ensure that the proposed transaction aligns with their existing country programmes and those of multilateral development institutions. For example, if the government is supported under an International Monetary Fund (IMF) programme, it is essential to ensure the transaction complies with the agreed-upon programme parameters and conditionalities.
Regulatory and Institutional Framework Alignment
17chap3_p_17When selecting financing instruments, it is crucial to ensure their alignment with the country’s statutory, legal, regulatory and institutional frameworks, thereby ensuring both effectiveness and sustainability.
18chap3_p_18All contracts and agreements should be duly authorised; legal, valid, binding and enforceable under national law as well as any applicable foreign law. They should clearly articulate the roles and responsibilities of the parties involved, their performance obligations, remedies for breaches, including any default or termination rights and incorporate an agreed-upon governing law and dispute resolution mechanism. This means that any proposed sustainability-linked instruments, debt swaps or PPP contracts should be permitted under existing frameworks or that such frameworks may need to be amended or supplemented.
19chap3_p_19Compliance with debt, fiscal and procurement laws should therefore be looked at critically. Debt instruments under consideration should fall within the limits and procedures established by relevant public finance management acts, debt management laws and public procurement frameworks. Some countries may require parliamentary and/or Cabinet approval, as well as listing in national budgets. Early consideration should be given to the approvals needed.
20chap3_p_20To address transparency and accountability issues, instruments should incorporate disclosure, auditing and oversight provisions to meet both domestic and international standards, as applicable in each case. Abiding by budget transparency principles or sectoral transparency tools (e.g. national health accounts) is also essential.
21chap3_p_21Whether through sustainable finance instruments, debt-for-health swaps or PPPs, governments should align disclosure practices with recognised international standards - such as the relevant International Capital Market Association (ICMA) and Loan Market Association (LMA) Principles for bonds and loans or the World Bank PPP Disclosure Framework for partnerships. This entails publishing key transaction terms, establishing appropriate governance and management of the funds raised, as well as regular performance and spend reports, capable of verification by independent reviewers when necessary. This can help trace how resources are mobilised, allocated and translated into measurable health outcomes.
22chap3_p_22Institutional capacity is another critical dimension: both lead ministries need adequate technical skills, operational systems, and coordination mechanisms to evaluate, manage and monitor the funding instruments and related contractual arrangements. Clarifying the roles of the MoF, specifically their existing debt management office or PPP unit, and that of the MoH, is critical, especially regarding who leads negotiations, execution and ongoing monitoring.
Intra-governmental Coordination
23chap3_p_23Every non-traditional and structured financing transaction, whether an SLF instrument, a debt swap or a PPP, cuts across fiscal, legal and sectoral mandates. Collaboration between ministries and agencies is therefore indispensable, not only for technical soundness but also for political and operational coherence.
24chap3_p_24The MoF and MoH should work together from the outset, jointly defining objectives, suitability of funding type, timelines and communication strategies. The MoF typically leads negotiations with banks, credit enhancement providers and investors, ensuring alignment with the country’s debt management strategy, budgetary cycle and the necessary technical expertise. Meanwhile, the MoH ensures that proposed activities are grounded in national health priorities and that health outcomes remain visible throughout the process. Suppose the transaction involves a third party implementing agreed health spend outcomes or programmes. In that case, the MoH should also lead on these aspects and the structure of any ongoing monitoring and reporting activities.
25chap3_p_25Because ministries have different mandates, each must see the value of the transaction through its own lens. The lead ministry should therefore frame messages in terms of the specific problems or concerns each counterpart is trying to solve, whether debt servicing elements for the MoF, service delivery performance for the MoH or legal safeguards for the Attorney General’s Office. This approach strengthens ownership and minimises resistance as discussions evolve.
26chap3_p_26Relevant MoF officials should include officials from the DMO and budget departments. In contrast, MoH representatives should consist of the Permanent Secretary, Head of Planning and relevant directorate leads, depending on the health programme or intervention being financed.
27chap3_p_27Other key public institutions may include:
- chap3_ul_0
- chap3_li_0The Office of the President or the Cabinet Office provides political backing and facilitates high-level decision-making.
- chap3_li_1The Attorney General’s Office ensures the transaction complies with national laws and provides legal opinions required as part of the transaction.
- chap3_li_2The Ministry of Planning and/or Economy aligns the transaction with national development priorities.
- chap3_li_3The National Statistics Office supports credible, timely and accurate reporting.
- chap3_li_4The Central Bank ensures consistency with foreign exchange management and monetary policy objectives.
- chap3_li_5The Ministry of Foreign Affairs is consulted specifically regarding bilateral debt swaps with other countries.
- chap3_li_6National health sector regulators are responsible for regulatory oversight, standards-setting, licensing, and compliance across the health system.
28chap3_p_28To support effective coordination across all stages of the transaction, countries may establish a dedicated intergovernmental committee with representatives from key institutions. The composition of this committee should reflect each country’s governance context, as there is no single model that fits all. For example, while the Office of the President may be listed here as a source of political support, in some countries, its early involvement is crucial to securing high-level buy-in and sustaining momentum. In other countries, the Office of the President has, through advisors, actually driven the transaction.
29chap3_p_29The list of potential members provided in this User Guide is therefore indicative, not prescriptive. Countries should adapt it to include any additional ministries, agencies or oversight bodies relevant to their context. To prevent duplication or reputational risk, the MoF and MoH should coordinate all external engagement through this mechanism, ensuring consistency, transparency and a unified national voice.
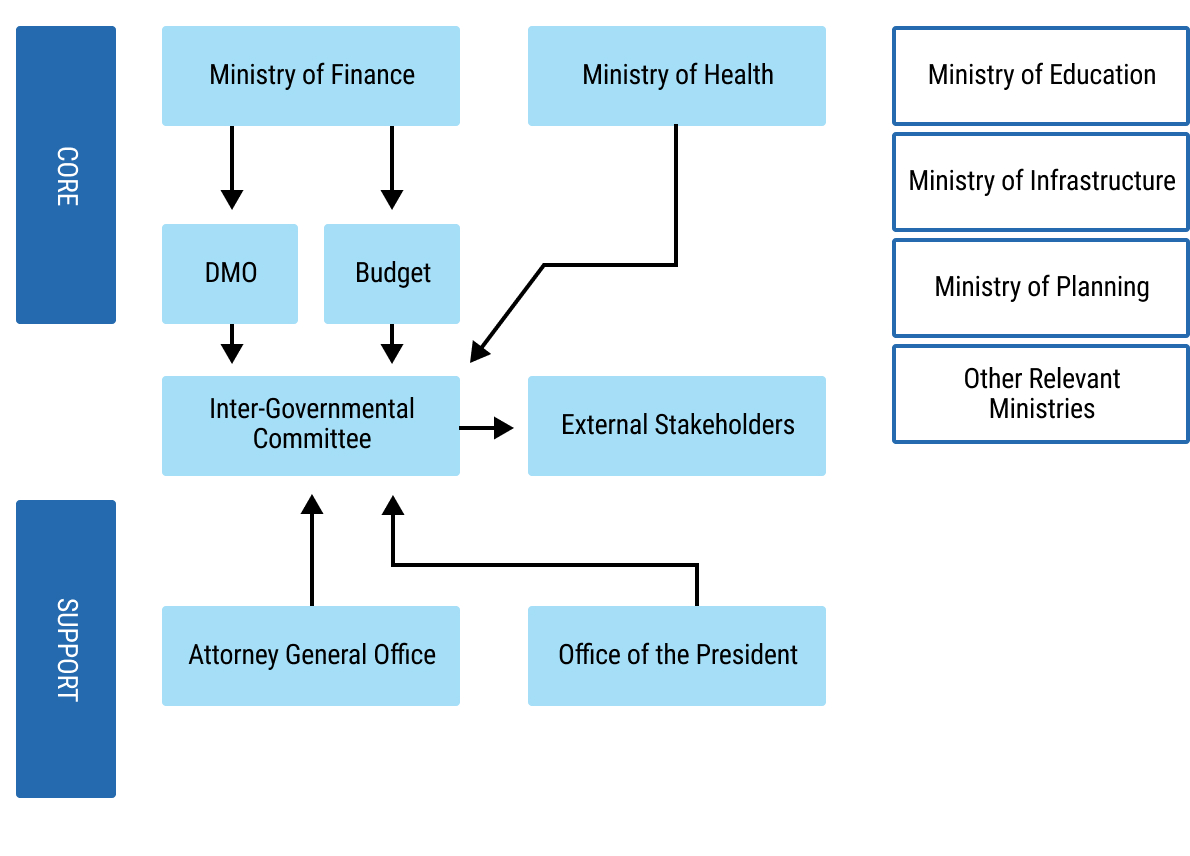 chap3_img_0
chap3_img_0External Stakeholder Engagement
30chap3_p_30In addition to inter-governmental coordination, early and regular engagement with the various external parties involved in the transaction can enhance credibility, mitigate political and reputational risk and reinforce the development impact.
31chap3_p_31Relevant external stakeholders encompass international institutions, the private sector and civil society actors. The engagement process would benefit from identifying dedicated officials within the intergovernmental coordination committee to engage with external partners regarding the envisaged transaction. These officials could include, for example, one person from the MoH and one from the MoF.
32chap3_p_32The following partners would need to be engaged, depending on the type of instrument and each at different parts of the process:
- chap3_ul_1
- chap3_li_7Global health institutions and partners can support activity design and implementation, including monitoring and reporting.
- chap3_li_8Banks and private investors would need to be tested to assess their appetite for the transaction and structure the financial parameters.
- chap3_li_9Credit enhancement providers can critically enable some of the financing structures presented in this User Guide. They can assess the feasibility of different financing structures, specify the availability of specific products and discuss the terms and conditions of their support.
- chap3_li_10Foreign governments, when considering bilateral debt swaps.
- chap3_li_11The IMF, the World Bank and other multilateral partners can ensure that the transaction aligns with the country’s programme objectives, if relevant, and, in the case of the IMF and World Bank specifically, is consistent with their debt sustainability assessments.
- chap3_li_12Credit rating agencies will need to be brought on board early to share relevant information and understand credit rating considerations.
- chap3_li_13Engaging private sector companies early on is crucial for PPPs to ensure early market sounding and transparent procurement, thereby attracting qualified operators and financiers.
- chap3_li_14Civil society organisations can input on the objectives of the transaction and help socialise the positive impact of the transaction.
- chap3_li_15The media can help ensure accurate reporting on the transaction and its health benefits.
Transparency and Communication Management
33chap3_p_33How governments communicate around financing mechanisms can be as important as the design of the mechanisms themselves. In the early stages, careful control of information is essential. Premature or poorly coordinated announcements can be easily misinterpreted by markets, creditors or rating agencies, potentially creating reputational, market and fiscal risks.
34chap3_p_34Confidentiality during the exploration and negotiation phases of any transaction allows the government to refine its proposal, align internal stakeholders and shape the narrative before it enters the public domain. Such confidentiality is vital in the case of commercial debt swaps involving the potential buyback of publicly traded bonds, as any announcement of a transaction could lead to a rally in the country’s bond prices, resulting in reduced fiscal savings from the debt swap. Once the design is finalised, transparency should take precedence. Public communication should focus on the transaction’s purpose, its alignment with national priorities and the mechanisms for accountability and reporting.
35chap3_p_35Effective communication strategies build confidence, both domestically and internationally. They signal that the government is managing innovation responsibly, safeguarding fiscal stability and ensuring that citizens and partners understand the rationale for new approaches to financing health.
36chap3_p_36Ideally, communication should evolve with the process: discreet and coordinated in early stages, open and transparent once agreements are finalised.
Building Country Ownership and Learning
37chap3_p_37The true legacy of any financing transaction should be a stronger national capacity. Beyond mobilising additional funds, each transaction provides an opportunity to build institutional knowledge, refine systems and strengthen governance.
38chap3_p_38Governments should document lessons learned, develop best practices, create templates and retain experienced teams to create continuity for future transactions. Over time, this institutional learning reduces transaction costs, accelerates timelines and increases national autonomy in managing complex financial instruments.
39chap3_p_39Every transaction, regardless of size, should therefore be seen not only as a means of mobilising resources but also as an investment in institutional capability. When capacity grows, credibility follows, and with it, greater access to sustainable financing opportunities in the future.
|
40chap3_p_40Debt management is consolidated at the DMO and governments should ensure that any fundraising, whether for health or other policy objectives, follows international best practices in public debt management. To support this, the IMF and World Bank have developed a set of voluntary principles to help debt managers strengthen institutional frameworks and reduce financial vulnerability. The key principles are summarised below:
41chap3_p_41For more details, the reader is referred to the Guidelines for Public Debt Management (2014) by the World Bank and IMF. |
Chapter 4: Health Finance and Key Performance Indicators
Key Takeaways
|
1chap4_p_1The remainder of this chapter provides the practical foundation for engaging with health financing instruments. It begins by outlining the global health institutions (GHIs), such as the Global Fund, Gavi, and the World Bank, that play a central role in shaping and supporting health investments across Africa, before summarising the major budget categories and types of activities commonly funded within the health sector. The chapter then introduces the key performance indicators (KPIs) that underpin many of the financing tools described in this User Guide. These indicators provide the measurable link between resources and results, helping governments structure agreements that reward progress, strengthen accountability, and align financial terms with tangible improvements in population health.
Setting Health Priorities
2chap4_p_2Governments set their health priorities through a combination of long-term planning processes and annual budget cycles. These processes are designed to align health goals with broader national development objectives, while ensuring that public resources are used effectively and transparently. For those engaging with the health sector - whether from Ministries of Finance (MoFs), development institutions, or debt management offices - understanding how these priorities are set is essential for navigating the financing landscape and identifying where different instruments can add value.
3chap4_p_3National Development Plans (NDPs) form the broadest and most strategic layer of this process. These 5- to 10-year visions outline a country’s economic and social transformation objectives, with health typically embedded as a core pillar of human capital development. They set the direction of travel: expanding access to essential services, improving the health workforce, strengthening disease control, or modernising infrastructure. While these plans are often ambitious, they signal government commitment and serve to provide an important reference point for investors and partners seeking alignment with national priorities.
4chap4_p_4Below the national vision sit sector-specific frameworks, most notably the national health sector strategic plans. These multi-year plans translate high-level aspirations into concrete priorities for the health system, defining service delivery goals, workforce needs, infrastructure requirements, digital health plans, and the reforms necessary to improve efficiency and equity. They guide Ministries of Health (MoHs) in preparing annual budgets, shaping investment cases, and coordinating support across development partners. Complementing these are targeted strategies for major disease areas or system needs, such as national HIV strategies, reproductive and maternal health plans, immunisation strategies, or human resources for health plans. These documents provide detailed, measurable targets that inform both government and partner financing decisions.
5chap4_p_5While these plans are comprehensive, not every activity is funded immediately. Each year, MoHs must translate their strategic priorities into an annual budget submission that reflects available fiscal space, existing commitments, and the realities of implementation capacity. As a result, long-term plans remain partly aspirational, with only a subset of priorities incorporated into the government budget at any given time. Understanding this pipeline, from long-term vision to sector strategies and annual budgets, is essential for anyone looking to support or finance health investments. It reveals not only what a country hopes to achieve, but also which priorities are ready for investment and which require sustained dialogue, planning, and resourcing. MoHs can use these costed and prioritised plans to make a case for inclusion in financing instruments.
International and Domestic Financing for Health
The Evolving Role of Global Health Initiatives
6chap4_p_6Global health institutions such as Gavi, the Global Financing Facility, and the Global Fund to fight AIDS, tuberculosis and malaria (Global Fund), have been instrumental in improving health outcomes and strengthening health systems across Africa. Although they continue to play a vital role, their focus is evolving. Increasingly, these institutions act not only as sources of grant financing but also as platforms for co-financing, technical support, and transition planning.
7chap4_p_7As countries move toward greater domestic resource mobilisation, GHIs are shifting from gap-fillers to enablers, helping governments design sustainable investment cases, align donor contributions with national priorities, and strengthen data and accountability systems. Their programmes now serve as building blocks for more integrated, country-led financing approaches, paving the way for mechanisms such as sustainability-linked loans, debt swaps, and PPPs to complement and reinforce existing health investments. The main active GHIs in Africa are treated below.
The Global Fund to Fight AIDS, Tuberculosis and Malaria
8chap4_p_8The Global Fund is a multilateral financing mechanism that mobilises and disburses resources to fight HIV/AIDS, tuberculosis and malaria, while strengthening health systems and
pandemic preparedness. It operates on a country-led model, meaning African governments and civil society set priorities through country coordinating mechanisms (CCMs). Countries that benefit from Global Fund support operate under a performance-based grant model, where country ownership plays a key role through the CCMs. Funds are channelled through Principal Recipients (e.g. MoHs, Non-Government Organisations (NGOs) or United Nations (UN) agencies). Global Fund programmes cover disease prevention, diagnosis, and treatment, and also strengthen health systems (supply chains, labs, community health workers).
Gavi, the Vaccine Alliance
9chap4_p_9Gavi focuses on routine immunisation, introducing new vaccines, and strengthening immunisation systems. It provides vaccine subsidies, and receiving countries contribute co-financing based on income level. Gavi utilises a pooled procurement system in collaboration with the United Nations Children’s Fund (UNICEF) Supply Division and the World Health Organisation (WHO) to negotiate vaccine prices and ensure supply security. Gavi develops multi-year immunisation plans and funds vaccine-delivery infrastructure (cold chain, logistics, digital systems, workforce training). A key feature is that, as countries become wealthier, they gradually assume full vaccine financing.
The Global Financing Facility (GFF)
10chap4_p_10The GFF, launched in 2015 and hosted by the World Bank, supports countries to improve reproductive, maternal, newborn, child, and adolescent health and nutrition (RMNCAH-N). It aims to catalyse domestic financing and align donor investments for long-term sustainability. Countries develop a national investment case - a prioritised plan linking health and nutrition goals with financing strategies that will define the GFF’s support as a combination of grant funding and World Bank loans. The GFF operates through a single national platform that unites ministries, donors, civil society, and the private sector under one financing framework.
11chap4_p_11The table below provides a summary of the focus areas and operating models for each of these entities. All three have significant links with MoHs and MoFs on the continent, although they often do not have staff based in country. Instead, they provide support through established, in-country governance mechanisms.
|
12chap4_p_12Global Fund |
13chap4_p_13Gavi |
14chap4_p_14Global Financing Facility |
|
|
15chap4_p_15Main function |
16chap4_p_16Disease programmes |
17chap4_p_17Preventive immunisation |
18chap4_p_18Health system financing backbone |
|
19chap4_p_19Core purpose |
20chap4_p_20HIV, TB, malaria, and health systems |
21chap4_p_21Vaccination and immunisation systems |
22chap4_p_22RMNCAH-N and health financing reform |
|
23chap4_p_23Delivery Model |
24chap4_p_24Grants via Country Coordinating Mechanisms (CCMs) |
25chap4_p_25Vaccine co-financing and supply partnerships |
26chap4_p_26Blended financing with World Bank loans |
|
27chap4_p_27Health System Role |
28chap4_p_28Funds workforce, labs, procurement, surveillance |
29chap4_p_29Builds immunisation cold chains, logistics, and data |
30chap4_p_30Strengthens health financing, data, and budgeting |
|
31chap4_p_31Key Implementers |
32chap4_p_32MoHs, NGOs, Civil Society, and UN agencies |
33chap4_p_33MoHs, NGOs, UNICEF, and WHO |
34chap4_p_34MoFs and MoHs, World Bank |
|
35chap4_p_35African Coverage |
36chap4_p_36~45 countries |
37chap4_p_37~40 countries |
38chap4_p_38~30 countries |
39chap4_p_39These institutions do not provide debt or credit enhancement solutions (see Chapter 7: The Use of Public-Private Partnerships in Healthcare Projects). However, they can play an essential convening role in designing financing instruments and in bringing together international and domestic stakeholders. They are a potential trustworthy partner to help create and monitor programme activities, providing credibility to in-country execution. Specifically, these institutions could act as third-party implementers for debt swaps (see Chapter 6: Debt-for-Health Swaps) and provide oversight on programme execution and data quality for sustainable debt instruments (see Chapter 5: Sustainable Finance Instruments).
Components of a Health Budget to be Financed
40chap4_p_40For MoFs and other financial planners, health budgets can sometimes appear complex - a mix of recurrent costs, capital investments, and programmatic expenditures that do not always align neatly with health objectives and outcomes. Yet, understanding the composition of health spending is crucial for identifying which areas are best suited to different financing solutions. Health systems rely on a range of inputs, including infrastructure, equipment, digital systems, healthcare workers, pharmaceuticals, energy and utilities, as well as service delivery contracts, training programmes, and community-based interventions. Each category carries distinct financing characteristics - some suited to long-term capital instruments, while others are suited to results-based or blended approaches.
41chap4_p_41The table below provides an overview of everyday activities within the health sector. It does not aim to be exhaustive, but rather to illustrate different elements of a typical health budget - such as infrastructure upgrades, supply-chain improvements, workforce investments, and preventive health programmes. Policymakers can identify the specific type of expenditures that require financing and match them with the appropriate financing tool, ensuring that limited resources are used strategically and sustainably.
|
42chap4_p_42Programme Type |
43chap4_p_43Example strategic priorities |
44chap4_p_44Description |
45chap4_p_45Added value for the MoF |
||
|
46chap4_p_46Capital Expenditure |
47chap4_p_47Operating Expenditure |
||||
|
48chap4_p_48Reproductive, maternal, newborn and child health 49chap4_p_49(Family planning, pregnancy care, immunisation, child treatment) |
50chap4_p_50Family planning service provision |
51chap4_p_51*Training the health workforce 52chap4_p_52*FP commodity procurement 53chap4_p_53*Behaviour change communication |
54chap4_p_54Reducing the birth rate will have downward pressure on health and education budgets |
||
|
55chap4_p_55Local manufacturing for immunisations |
56chap4_p_56*Construction of a factory |
57chap4_p_57*Input costs 58chap4_p_58*Running costs |
59chap4_p_59Potential taxation and employment generation |
||
|
60chap4_p_60Immunisation service delivery |
61chap4_p_61*Procurement of cold chain equipment (fridges, etc.) |
62chap4_p_62*Procurement of vaccines 63chap4_p_63*Vaccination campaigns 64chap4_p_64*Improving data systems for tracking 65chap4_p_65*Staff training |
66chap4_p_66Strong immunisation programme reduces cost and supports pandemic preparedness |
||
|
67chap4_p_67Infectious Diseases 68chap4_p_68(TB, HIV, malaria, water & sanitation, neglected tropical diseases) |
69chap4_p_69Disease elimination campaigns |
70chap4_p_70*Investments in laboratory capacity (I.e. equipment/lab sites) |
71chap4_p_71*Data and tracking systems improvements 72chap4_p_72*Surveillance systems 73chap4_p_73*Delivery of prevention and treatment activities (e.g. bed nets, trachoma surgeries) |
74chap4_p_74Disease elimination reduces treatment costs and increases workforce productivity. |
|
|
75chap4_p_75HIV treatment integration |
76chap4_p_76*Investment in testing equipment (CD4 / Viral Load) |
77chap4_p_77*Training of staff 78chap4_p_78*Data systems improvements 79chap4_p_79*Procurement of test and treatment commodities 80chap4_p_80*Behaviour change |
81chap4_p_81Successful HIV treatment reduces the transmission of HIV and improves workforce productivity |
||
|
82chap4_p_82Service capacity and access 83chap4_p_83(Health workforce, hospital access, health facility availability, pandemic preparedness) |
84chap4_p_84Construction of new hospitals/health centres to increase access to services |
85chap4_p_85*Hospital/health centre construction 86chap4_p_86*Equipment procurement |
87chap4_p_87*Salaries for hospital staff 88chap4_p_88*Running costs (I.e. utilities) |
89chap4_p_89The construction of hospitals should be considered in the context of spending on preventive care to understand the value for money. |
|
|
90chap4_p_90Health workforce and community health workforce development |
91chap4_p_91*Construction of staff housing |
92chap4_p_92*Salaries for the workforce (including community health workers) 93chap4_p_93*Ongoing training for quality and retention 94chap4_p_94*Incentives/benefits 95chap4_p_95*Pre-service training (I.e. cost of universities) |
96chap4_p_96Moving community health workers into the salaried workforce has a substantial impact on prevention activities and the improvement of health service delivery. |
||
|
97chap4_p_97Pandemic preparedness |
98chap4_p_98*Procurement of laboratory systems |
99chap4_p_99*Coordination mechanism for disease monitoring across animal and human health 100chap4_p_100*Staff trainings 101chap4_p_101*Surveillance (I.e. travel to outbreaks) 102chap4_p_102*Salary for public health institutions (e.g. CDC) 103chap4_p_103*Develop a sample transportation system for lab testing 104chap4_p_104*Strengthen data systems for tracking and surveillance |
105chap4_p_105Pandemic preparedness is essential to respond to localised outbreaks and potential epidemics/pandemics |
||
Key Performance Indicators for Health
Role of Key Performance Indicators for Sustainable Health Financing
106chap4_p_106KPIs are key components for sustainable finance instruments, debt swaps and PPPs. For sustainably-linked financing instruments (SLFs) (I.e. sustainability-linked loans (SLLs) and sustainability-linked bonds (SLBs)), the KPI target describes which health aspect the instrument targets and links the setting of interest rates relative to achieving the sustainability performance targets (SPTs) for the relevant KPI, such that:
- chap4_ul_1
- chap4_li_5If the issuer achieves the KPI target, they will benefit from lower interest rates.
- chap4_li_6Conversely, they will face higher interest rates if they fail to meet the KPI target.
107chap4_p_107Hence, a key component of SLFs is the monitoring, reporting, and verification (MRV) system, which tracks the progress of KPIs throughout the instrument’s lifetime (see Chapter 5: Sustainable Finance Instruments).
108chap4_p_108In debt swaps, KPIs serve as safeguards to ensure that commitments made available through debt reductions are utilised to support projects and initiatives that improve health outcomes. Similar to SLFs, KPI tracking helps creditors verify the impact and therefore shape the scale and acceptability of the debt swap. If these commitments are not fulfilled, issuers will face recourse through contractually agreed-upon remedies (see Chapter 6: Debt-for-Health Swaps).
109chap4_p_109In PPPs, KPIs also serve to incentivise the longevity of the asset and good operational performance. This requires monitoring implementation and operations through the Contract Monitoring Regime, ensuring that parties continue to bear the risk allocation specified in the PPP Agreement (see Chapter 6: Debt-for-Health Swaps).
Principles of KPI Selection for Sustainable Debt Instruments
110chap4_p_110The selection of KPIs is critical for setting goals and incentives for the issuers. This is particularly evident for SLFs, where the achievement of KPIs has a direct impact on the cost of debt; however, the same criteria apply to health bonds, loans, and debt swaps. Developing health KPIs that are economically and financially material for a government can positively affect the whole economy in the long term.
111chap4_p_111While not a focus of this chapter, it is worth mentioning that, in addition to the KPI selection, the carrots and sticks of an SLF ultimately depend on its SPT (see Box A on the following page). This target-setting exercise is not trivial and must be conducted with the country’s own economic context, priorities, history, and peers in mind. One way to identify strong targets is to use the Feasibility and Ambitiousness (FAB) framework, developed by the World Bank. The FAB dashboard is a tool that enables users to conduct an assessment for a KPI of their choice, provided it is covered in the World Bank’s Sovereign Environmental, Social and Governance (ESG) Data Portal.
112chap4_p_112Four key dimensions should be considered when selecting a KPI for these instruments:
113chap4_p_113Controllability. KPIs serve a dual purpose. First, they define what indicator the instrument aims to improve, which is then formalised as the SPT. Second, they set the carrots and sticks (see Box A on the following page) for the issuer to ensure the SPT is reached. The controllability principle (see Nobel Prize lecture by Bengt Holmström (2016) on Pay for Performance and Beyond) is a helpful guideline for selecting KPIs, as the MoH will be unlikely to commit to a target if the outcome is driven mainly by outside or predetermined factors, such as life expectancy, and not only influenced by national policy action. The concept of controllability is closely related to attributability described in Flugge et al. (2021)
Box A: The “Carrots and Sticks” of Sustainability-Linked Financing114chap4_p_114The controllability principle states that KPIs in SLFs should reflect outcomes that the issuer can meaningfully influence. For governments, this principle is central because they are risk-averse and accountable for the use of taxpayer resources. If a KPI is heavily driven by external shocks, such as global food prices or extreme weather, the government may face financial penalties despite taking all reasonable policy actions. This reduces willingness to issue sustainability-linked instruments and weakens the credibility of the financing structure. 115chap4_p_115To address this, KPIs should be selected or constructed to isolate the portion of performance that is within governmental control. For example, suppose a government aims to improve nutrition outcomes. In that case, the metric should be defined in a way that removes exogenous price effects or focuses on controllable drivers such as distribution efficiency, targeted safety-net coverage, or domestic programme delivery. Designing KPIs in this way protects the issuer from uncontrollable volatility, aligns incentives between the government and investors, and increases the feasibility of adopting SLF at scale. 116chap4_p_116(For an explanation of the controllability principle in the context of nutrition-related KPIs, see Wang and de Smit (2026, forthcoming),Wang and de Smit. (2026, forthcoming). Sustainability-Linked Financing with Health KPIs in Africa. World Bank Policy Research Working Paper. or in the context of forestry KPIs, see Wang et al (2023).) |
117chap4_p_117Observability. KPIs require annual observation frequencies that can be reported and verified. Ideally, these KPIs have historical data and comparable data in peer countries. Measurement errors need to be accounted for, as they may lead to SPTs or commitments being reached or broken despite being within the margin of error of surveys. Box B describes the specific challenges when relying on KPIs that use modelled estimates.
118chap4_p_118Absolute or relative measures. KPIs are often available in two formats. First, in absolute numbers (e.g. number of nurses) and second, in relative terms (e.g. number of nurses per 100,000 population). The former tends to be more accurate as the denominator of the second (e.g. population statistics) may come from a different source and introduce new sources of measurement errors and survey uncertainties. However, the benefit of relative numbers is that it facilitates comparison with peer countries.
Box B: Challenges with health KPIs based on modelled estimates119chap4_p_119A recurring challenge in health-sector KPIs is that the underlying data are often sparse, noisy, or inconsistent across sources. To address these limitations, international agencies publish modelled estimates that systematically fill data gaps and produce long-run trajectories that are internally consistent across time and countries. These approaches impose a degree of smoothness on the data and aim at identifying generalisable trends across countries. Before the issuance of the debt instrument, this stability can help characterise a business-as-usual (BAU) trajectory and serve as a benchmark against which future progress or policies can be assessed, without allowing single irregular observations to skew the picture (see the blue line in the figure below).  chap4_img_0 chap4_img_0120chap4_p_120After the debt is issued, during monitoring and evaluation, these same properties can make modelled estimates inappropriate for use as KPIs. KPIs are intended to track meaningful departures from the BAU path. Yet, modelled estimates are designed to down-weight abrupt changes, even when those changes may reflect genuine policy action or structural shifts. Smoothing techniques such as penalised splines or mixed-effects models are used with the explicit intention of limiting volatility and outliers. While these methods eventually adjust to new patterns that persist, they are not designed to capture rapid movements that may be critical for assessing the outcomes of policy change. For this reason, when evaluating impacts or determining the achievement of SPTs, alternative data sources such as unmodelled survey data can provide a clearer signal of real-time change (see the last red dot in the figure above). However, we should note that survey data can carry its own uncertainties. For details, see Wang and de Smit (2026, forthcoming). |
121chap4_p_121Frequency and lag. The KPIs should be observed at least annually. If the KPIs are reported with a significant lag, it will introduce complications with the carrot and sticks (see Case Study below), which in turn weakens the financial incentive structures. The lag should also account for the time necessary to verify the KPIs.
Examples of Health KPIs for Sustainable Debt Instruments
122chap4_p_122Unless the sustainable debt instruments are used to fund a specific PPP project, health KPIs for SLFs, use of proceeds (UoPs), and debt swaps typically address system-wide issues. This section describes three health KPIs in the context of the lifecycle of a health outcome, starting from the high-level national policy, to the observable activities, outputs and outcomes, and the final impact measure. We also describe the suitability of the three financial instruments for each step of the health improvement journey, borrowing the terminology of the Donabedian framework.
123chap4_p_123The examples provided below were chosen to be illustrative. The indicators chosen for debt instruments will need to be considered and evaluated on a case-by-case basis, in line with the country’s context, health priorities, and data availability and quality. For example, indicators on TB, immunisation or health facility access could equally be considered, based on data availability.
124chap4_p_124As seen in the examples below, health bonds and loans are typically aligned with activity-level interventions, which can be easily mapped and tracked within the budget. Investors in an SLF are generally interested in more outcome- or impact-oriented data; however, the MoH must propose indicators that are within their control to influence and that have strong data systems capable of regular updates. Debt swaps are the most versatile instrument and can incorporate KPIs from different levels, including policy or legal commitments from the government. As with SLFs, they will require strong data systems that can be monitored and verified for each indicator.
|
125chap4_p_125Step |
126chap4_p_126Policy Commitment |
127chap4_p_127Process |
128chap4_p_128Outcome |
||
|
129chap4_p_129KPI / Policy |
130chap4_p_130Plan to integrate HIV test and treatment into the benefit package and national insurance plan |
131chap4_p_131Number of health workers trained in HIV testing and treatment |
132chap4_p_132Number of people tested for HIV 133chap4_p_133Number of people on Treatment |
134chap4_p_134% of people on ART who achieved viral suppression |
135chap4_p_135HIV new incidence rate |
|
136chap4_p_136Controllability |
137chap4_p_137High |
138chap4_p_138High |
139chap4_p_139High |
140chap4_p_140High |
141chap4_p_141Medium |
|
142chap4_p_142Observability |
143chap4_p_143High |
144chap4_p_144High |
145chap4_p_145Medium |
146chap4_p_146Medium |
147chap4_p_147Low |
|
148chap4_p_148Health Bond/Loan |
149chap4_p_149❌ |
150chap4_p_150✅ |
151chap4_p_151❌ |
152chap4_p_152❌ |
153chap4_p_153❌ |
|
154chap4_p_154SLF |
155chap4_p_155❌ |
156chap4_p_156❌ |
157chap4_p_157✅ |
158chap4_p_158✅ |
159chap4_p_159❌ |
|
160chap4_p_160Debt Swaps |
161chap4_p_161✅ |
162chap4_p_162✅ |
163chap4_p_163✅ |
164chap4_p_164✅ |
165chap4_p_165❌ |
166chap4_p_166Reduction of HIV incidence rate (Table 4.3). In the case of HIV, the incidence rate may not be ideal for the SLF instrument or debt swap in cases where it relies on prevalence surveys that are not conducted annually. Where data quality is strong for the number of people tested and treated for HIV or the % of people on antiretroviral therapy (ART) who are virally suppressed, these could serve as strong KPIs for SLF and debt swaps.
|
167chap4_p_167Step |
168chap4_p_168Policy Commitment |
169chap4_p_169Process |
170chap4_p_170Outcome |
||
|
171chap4_p_171KPI / Policy |
172chap4_p_172Health workforce development plan addressing key challenges (retention, brain drain) |
173chap4_p_173Number of health colleges built, and students enrolled 174chap4_p_174(in collaboration with the Ministry of Education) |
175chap4_p_175Number of doctors/nurses per 1,000 population |
176chap4_p_176Retention rate for public health workers |
177chap4_p_177Patient satisfaction surveys (measuring quality of care) |
|
178chap4_p_178Controllability |
179chap4_p_179High |
180chap4_p_180High |
181chap4_p_181Medium |
182chap4_p_182Medium |
183chap4_p_183Medium |
|
184chap4_p_184Observability |
185chap4_p_185High |
186chap4_p_186High |
187chap4_p_187High |
188chap4_p_188Medium |
189chap4_p_189Low |
|
190chap4_p_190Health Bond/Loan |
191chap4_p_191❌ |
192chap4_p_192✅ |
193chap4_p_193❌ |
194chap4_p_194❌ |
195chap4_p_195❌ |
|
196chap4_p_196SLF |
197chap4_p_197❌ |
198chap4_p_198✅ |
199chap4_p_199✅ |
200chap4_p_200❌ |
201chap4_p_201❌ |
|
202chap4_p_202Debt Swaps |
203chap4_p_203✅ |
204chap4_p_204✅ |
205chap4_p_205✅ |
206chap4_p_206✅ |
207chap4_p_207❌ |
208chap4_p_208Improving the access to and quality of the health workforce (Table 4.4). In this example of the health workforce, the indicators available for the SLF may be more limited. Given that the retention rate is complex to influence and even more challenging to monitor (due to limitations in the HRIS data system), the outcome indicator may not be suitable for the SLF. However, the ratio of doctors or nurses to the population could be a good option, as this is an internationally recognised indicator with reasonably robust underlying data.
209chap4_p_209The retention rate may be selected for the debt swap. If this is a key priority for the government, additional indicators or support will be provided to improve data quality on this indicator.
|
210chap4_p_210Step |
211chap4_p_211Policy Commitment |
212chap4_p_212Process |
213chap4_p_213Outcome |
||
|
214chap4_p_214KPI / Policy |
215chap4_p_215Guidelines produced to promote exclusive breastfeeding |
216chap4_p_216Number of School-based deworming campaigns run |
217chap4_p_217Number of children who have taken deworming treatment |
218chap4_p_218Prevalence of under-5 stunting |
219chap4_p_219Under-5 mortality rate |
|
220chap4_p_220Controllability |
221chap4_p_221High |
222chap4_p_222High |
223chap4_p_223High |
224chap4_p_224Low |
225chap4_p_225Low |
|
226chap4_p_226Observability |
227chap4_p_227High |
228chap4_p_228High |
229chap4_p_229High |
230chap4_p_230Medium |
231chap4_p_231Medium |
|
232chap4_p_232Health Bond/Loan |
233chap4_p_233❌ |
234chap4_p_234✅ |
235chap4_p_235❌ |
236chap4_p_236❌ |
237chap4_p_237❌ |
|
238chap4_p_238SLF |
239chap4_p_239❌ |
240chap4_p_240❌ |
241chap4_p_241✅ |
242chap4_p_242❌ |
243chap4_p_243❌ |
|
244chap4_p_244Debt Swaps |
245chap4_p_245✅ |
246chap4_p_246✅ |
247chap4_p_247✅ |
248chap4_p_248❌ |
249chap4_p_249❌ |
250chap4_p_250Improving children’s health and nutrition (Table 4.5). In this example for child nutrition and under-five mortality rate, the country may not feel confident in its ability to influence under-5 stunting with a health-only intervention, as this is a multi-sectoral effort. Additionally, data collection methods for this indicator, as well as the under-5 mortality rate, rely on surveys and may not be updated frequently enough to be used in an SLF or debt swaps. In this case, focusing on the provision of services, such as deworming campaigns or deworming coverage, may be preferable, provided there is strong data availability.
Further Examples of Health KPIs
251chap4_p_251The KPIs shown above are selected from a larger set of health-related KPIs provided by the WHO. They are indicative examples. Countries should consider their own data and priorities when identifying KPIs that are appropriate for their specific financing instruments.
252chap4_p_252A comprehensive list of KPIs is forthcoming from Wang and de Smit (2026)Wang and de Smit. (2026, forthcoming). Sustainability-Linked Financing with Health KPIs in Africa. World Bank Policy Research Working Paper. identifying a shortlist of standardised health indicators that satisfy a set of data availability criteria, which include temporal coverage, country coverage, average and median lag, controllability, and observability for countries in Latin America, sub-Saharan Africa and the Asia Pacific.
Principles of KPI Selection for PPPs
253chap4_p_253PPPs are fundamentally concerned with the transfer of risk. If the private partner does not manage their operations effectively, they may incur financial losses in the form of penalties and payment deductions. If this persists, they may also face termination of their contract. This is typically incorporated into the payment and performance quality regime for a PPP, which generally addresses two matters: the availability of the facility and the quality of services being delivered.
254chap4_p_254Measurement is conducted through a series of quality indicators (QIs), with availability assessed through technical and operational tests (referred to as availability indicators (AIs)), which determine whether a health facility (e.g. a hospital, laboratory, hospital wing, or health centre) is available or not. As availability payments are, by definition, made for the available facilities, this means that part or all of the availability payment is at risk if the private partner does not keep the entire facility available at all times.
255chap4_p_255Performance is measured through a series of performance indicators (PIs), some of which are generic (e.g. infection control) and others that are specific to the facility’s clinical services profile (e.g. cardiology-specific PIs). If the private partner persistently fails to meet some or all of its PIs, it can stand the risk of the PPP Agreement being terminated.
256chap4_p_256The most critical patient safety and clinical outcome parameters are used to calculate and apply payment deductions from the due payments. These are referred to as KPIs.
257chap4_p_257Therefore, the selection of AIs, PIs, and KPIs is critical for setting goals and incentivising good performance. AIs, PIs and KPIs need to be realistic and representative, reflecting safety and quality of care standards. If QIs are set too harshly, they can render a PPP transaction unbankable or significantly impact the risk margins and/ or cost of capital. This is because harsh QIs can attract significant penalties and payment deductions. It is therefore advisable to set the measures, drawing on realistic practical experience, and to incorporate alongside them a realistic notification and rectification regime, which at the same time safeguards patient and people safety. Financial modelling is used to calibrate the penalty deduction mechanism and set the penalty deduction quantum such that the financial impact on the private partner is limited.
Chapter 5: Sustainable Finance Instruments
Key Takeaways
|
1chap5_p_1This chapter aims to guide officials from Ministries of Finance (MoFs) and Ministries of Health (MoHs), as well as practitioners, on the design and implementation of sustainable financing instruments - specifically UoP and sustainability-linked bonds (SLB) and sustainability-linked loans (SLL) - as mechanisms to mobilise public and private capital for health objectives. These instruments represent two complementary approaches to integrating sustainability into financing strategies: one through the earmarking of funds for eligible health-related projects (the UoP approach), and the other by linking financial terms to measurable health and sustainability performance (the sustainability-linked approach).
2chap5_p_2Three types of financing instruments are covered in this section:
- chap5_ul_1
- chap5_li_5Health bonds and loans. Models based on the UoP approach and would require the country to earmark the funds raised towards health projects and activities, such as infrastructure development or disease-specific programmes. This commitment will be contractually binding and must be reflected in the mandatory annual allocation reports. Therefore, robust project selection, transparent fund management and rigorous reporting are essential to ensure that resources achieve their intended outcomes and to maintain investor confidence.
- chap5_li_6SLBs and SLLs. Instruments in which the cost of financing is directly contingent upon the achievement of predefined sustainability targets. In the health sector, these targets could include expanding access to essential health services through improved health workforce availability or the expanded utilisation of quality services, such as for human immunodeficiency virus (HIV) patients with suppressed viral loads. When targets are met or exceeded, issuers benefit from more favourable financial terms; conversely, underperformance triggers penalties or adjustments, thereby incentivising continuous improvement.
- chap5_li_7Impact bonds. Performance-based approach bonds involving contractual arrangements between a government and/or donor and investors. In these arrangements, the government and/or donor commit to making payments contingent on the achievement of pre-agreed outcomes, specifically health-related objectives. These instruments typically operate on a more limited scale, but still offer a targeted mechanism for linking financing to measurable impact.
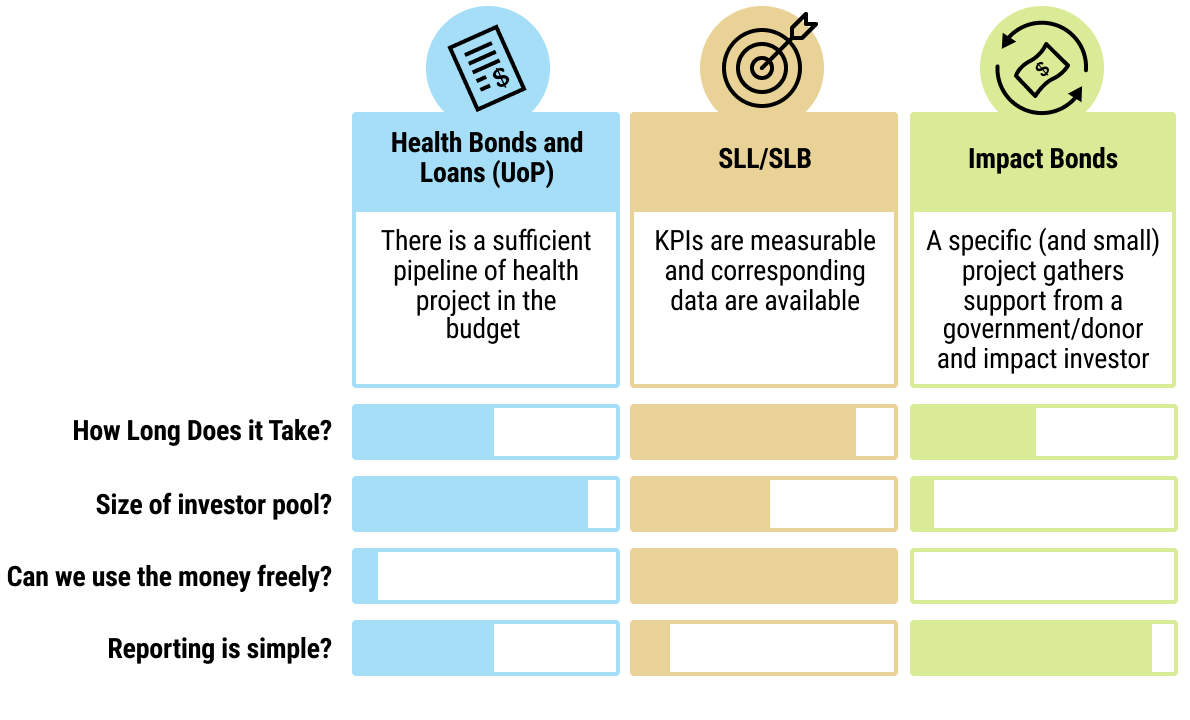 chap5_img_0
chap5_img_0
Financing Sustainable Health
3chap5_p_3Globally, the issuance of these instruments has grown rapidly in emerging markets, with UoP structures still dominating the market. Sustainability-linked financing, although less common, is gaining traction as performance-based mechanisms are seen to reflect progress toward national sustainable development goals better. In Africa, over 150 sustainable UoP bonds have been issued in both foreign and local currencies, totalling more than USD 15 billion. South Africa, Nigeria, Egypt and Côte d’Ivoire lead in terms of volume and diversity of instruments. A notable milestone occurred in August 2025, when Côte d’Ivoire issued Africa’s first foreign currency-denominated sustainability-linked loan, supported by the World Bank.
4chap5_p_4International financial institutions and development banks increasingly promote these instruments for their potential to channel private capital into sustainable development across the region. Together, they offer governments and health authorities practical tools to mobilise private resources while aligning debt management strategies with national development and sustainability objectives.
Health Bonds and Loans (UoP)
Case Study: Differences Between Bonds and Loans5chap5_p_5Throughout this chapter, reference to two distinct debt instruments will be made: (i) loans and (ii) bonds.
6chap5_p_6Summary of main differences
22chap5_p_22For further details of the range of creditor types, instruments and financing structures, see the African Legal Support Facility’s (ALSF) handbook Understanding Sovereign Debt: Options and Opportunities for Africa. |
Description and Rationale
23chap5_p_23Unlike traditional debt instruments that finance general budget needs, UoP bonds and loans allocate funds to projects with clear environmental or social benefits. There are three main types.
- chap5_ul_3
- chap5_li_10Green bonds/loans. Finance environmental initiatives (e.g. renewable energy, forestry, marine conservation).
- chap5_li_11Social bonds/loans. Support social programmes (e.g. healthcare, education, gender equality).
- chap5_li_12Sustainable bonds/loans. Combine both environmental and social objectives.
24chap5_p_24A health bond or loan would fall under the social category, funding health-related expenditures such as hospital construction, medical equipment purchases, vaccination programmes and improved access to care.
25chap5_p_25UoP instruments are not new - they have been widely used for years by governments, development banks and corporations, including in Africa. They operate under internationally recognised guidelines set by two key market bodies: the International Capital Market Association (ICMA) for bonds and the Loan Market Association (LMA) for loans. These guidelines are, in principle, voluntary, but in practice, it is highly recommended to follow them.
26chap5_p_26For sovereign borrowers, UoP instruments offer four significant benefits:
- chap5_ul_4
- chap5_li_13Alignment with global standards. Clear, comprehensive and regularly updated guidelines enhance transparency and credibility.
- chap5_li_14Reputation building. Health bonds and loans generate positive visibility, allowing governments to showcase their development strategies and highlight ongoing policies and projects.
- chap5_li_15Investor confidence. These instruments are familiar to investors, who value the assurance that funds are earmarked for specific, budget-identified projects aligned with social goals.
- chap5_li_16Unlocking new funding sources. UoP issuance attracts investors focused on social impact and taps into environmental, social and governance (ESG)-dedicated funding sources.
Enabling Conditions
27chap5_p_27The following enabling conditions establish the institutional and operational foundation necessary to support a credible and successful health bond issuance or loan contraction.
28chap5_p_28High-level political buy-in. Strong political leadership is indispensable to overcoming bureaucratic barriers and facilitating cooperation across ministries, agencies, and government departments. Issuing and managing health loans and bonds throughout their life cycle requires a high degree of inter-ministerial coordination, which can be challenging without a political champion, typically originating from either the MoH or the MoF (for example, the head of the debt management office (DMO)).
29chap5_p_29Conducive legal and regulatory frameworks. A country’s statutory, legal and regulatory framework defines how public borrowing is authorised and managed. It typically covers borrowing approvals, parliamentary oversight, debt contracting and recording procedures and limits on government borrowing or guarantees. For health bonds or loans, national frameworks must allow - or at least not prohibit - earmarked borrowing for specific purposes, such as health programmes. If the legal framework is silent or unclear, governments should consider amending laws to explicitly authorise debt for defined policy objectives (e.g. health). Such clarity reduces legal risk and strengthens investor confidence in the legitimacy and enforceability of the instrument.
30chap5_p_30Experience and market readiness. Countries with experience issuing foreign-currency bonds or contracting external loans are generally better positioned to adopt a UoP framework for health. While prior issuance of conventional debt is not a requirement, it helps build investor relationships - a sound foundation before moving to more specialised instruments like health-linked debt. Regardless of experience, early engagement with international investors is critical. This dialogue helps clarify their expectations, particularly around which health expenditures are most attractive to the market. These insights allow governments to design the structure of the operation in a way that maximises investor interest and confidence.
31chap5_p_31Sufficient project and expenditure pipeline. Before issuing a health bond or loan, the government needs to identify a sufficiently large amount of eligible health expenditures in its budget to match the target amount of the new debt. Typically, for a health bond in the international capital markets, a country would ideally identify health-related projects/programmes requiring funding from the national budget of at least USD 500 million, typically spent over 2-3 years. Smaller transactions could nevertheless be privately placed in the bond markets with a smaller group of investors or funded through loans. It is important to note that governments retain flexibility on the list of expenditures to be financed by the new debt instrument:
- chap5_ul_5
- chap5_li_17Multi-year allocation. Eligible expenditures can span several fiscal years. For example, a bond issued in 2026 can cover past (2025) and future (2026-2028) health spending.
- chap5_li_18Adjustable list. The exact list of expenditures does not need to be finalised at issuance. Governments can update it later during the subsequent reporting phase, based on actual budget execution.
- chap5_li_19Broader scope. Expenditures do not have to be limited to health: governments could opt for a broader social bond or loan, where health can be combined with other social sectors (e.g. education).
Opportunities and Challenges
Opportunities
- chap5_ul_6
- chap5_li_20Significant issuance potential. UoP instruments can mobilise substantial financing volumes, particularly when structured as a bond issued on international markets.
- chap5_li_21Market familiarity. Based on well-established ICMA and LMA frameworks, UoP bonds and loans are easily understood by investors, enhancing demand.
- chap5_li_22Visibility and credibility. Linking borrowing to health-related expenditures strengthens the government’s social commitment and improves investor confidence. A case can even be made that increased health expenditures can support economic growth and, ultimately, debt sustainability.
- chap5_li_23Access to a broader pool of investors. Socially responsible and ESG investors are more likely to participate in addition to the existing investor base, increasing the chances of success for these instruments.
Challenges
32chap5_p_32Complex transaction preparation. Developing a dedicated national social or health bond or loan framework aligned with relevant standards like ICMA or LMA takes time and coordination across key ministries (e.g. MoH). It is resource-intensive and demands strong administrative commitment and technical capacity. In addition, identifying sufficient eligible expenditures in the budget to meet the minimum transaction size (especially for bonds) might be challenging for some countries.
33chap5_p_33Firm reporting commitments. Borrowers must report annually on how proceeds are used until all funds are allocated. Reports detail financed programmes and may showcase flagship projects with expected impacts. While not mandatory, investors often request third-party audits for added assurance. This process can be demanding and requires close collaboration between the DMO, the budget department and relevant ministries (I.e. the MoH). Meeting these standards on time is crucial to establishing credibility as an ESG issuer and enhancing future market access. Importantly, reporting requirements can be legally binding - failure to comply may trigger events of default with serious consequences for the country.
Implementation
34chap5_p_34Issuing a UoP debt instrument will require thorough preparation and specific execution workstreams compared to more standard debt instruments. Figure 5.3 below summarises a checklist of all activities that need to be conducted through the process.
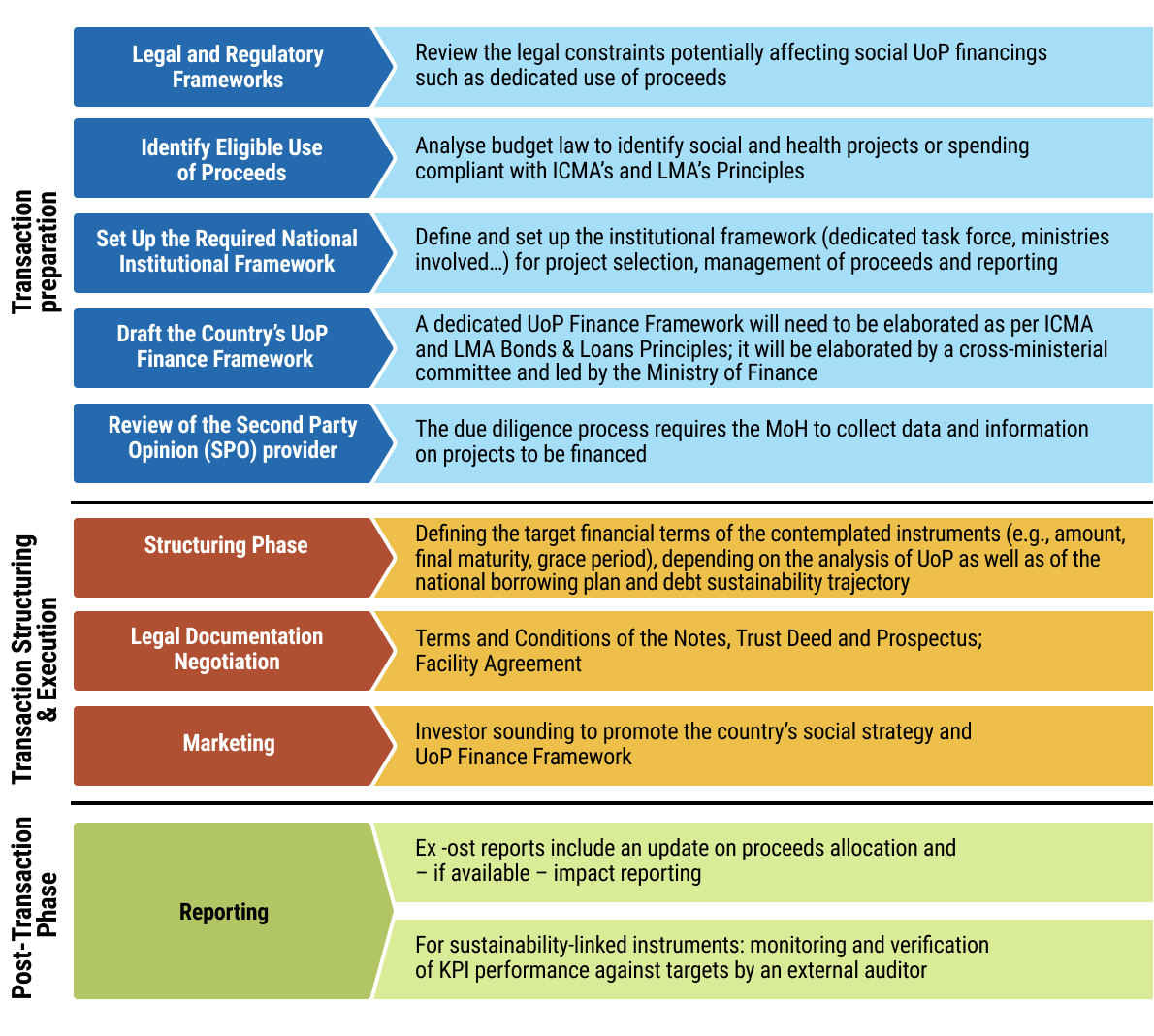 chap5_img_1
chap5_img_1
35chap5_p_35Across this process, three elements are core to UoP debt financing.
- chap5_ol_0
- chap5_li_24Preparation of a dedicated UoP Finance Framework for health. If the ICMA or LMA guidelines are being followed, the national framework will be mandatory for any borrower that wants to issue a UoP debt instrument on the international markets. The Framework serves as the reference for all future UoP issuances. It aims at (i) presenting the country’s national social and/or health priorities, (ii) defining clear eligibility criteria to select expenditures and projects financed by UoP instruments (e.g. health-related spending), and (iii) presenting the country’s governance structure in charge of selecting eligible expenditures and managing reporting. Such Frameworks need to be reviewed by an external third party, which will provide a second party opinion (SPO) confirming the document’s alignment with international standards. The Case Study below details the content and format of a UoP Finance Framework.
Case Study: Format and Content of a UoP Finance Framework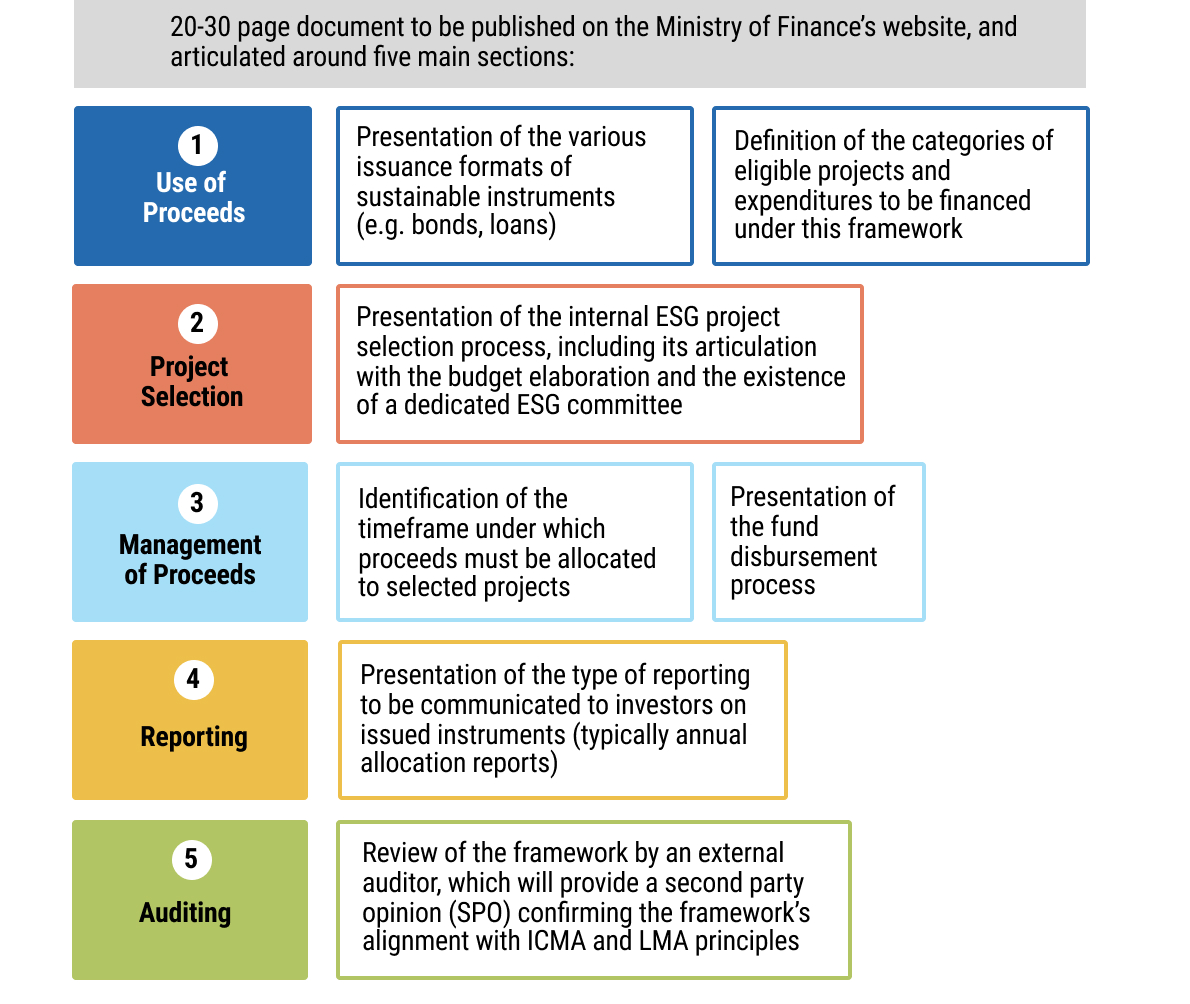 chap5_img_2 chap5_img_2 |
- chap5_ol_1
- chap5_li_25Extensive stakeholder engagement. Health bonds and loans require coordination among various key stakeholders throughout the process (see example of France in the Case Study below). The MoF and its DMO typically lead the process, ensuring alignment with government priorities and managing structuring and negotiations with investment banks and advisors. The MoH provides sector expertise, confirming that the proposed health-related eligibility criteria outlined in the UoP Finance Framework align with existing health plans. The Attorney General’s office or the Ministry of Justice ensures legal compliance by issuing necessary approvals and opinions. To streamline this complex process, it is recommended that a dedicated task force be created to oversee each step and maintain coordination among all parties.
Case Study: Example of the French UoP Bond - Selection of Eligible Expenditures and Interministerial Coordination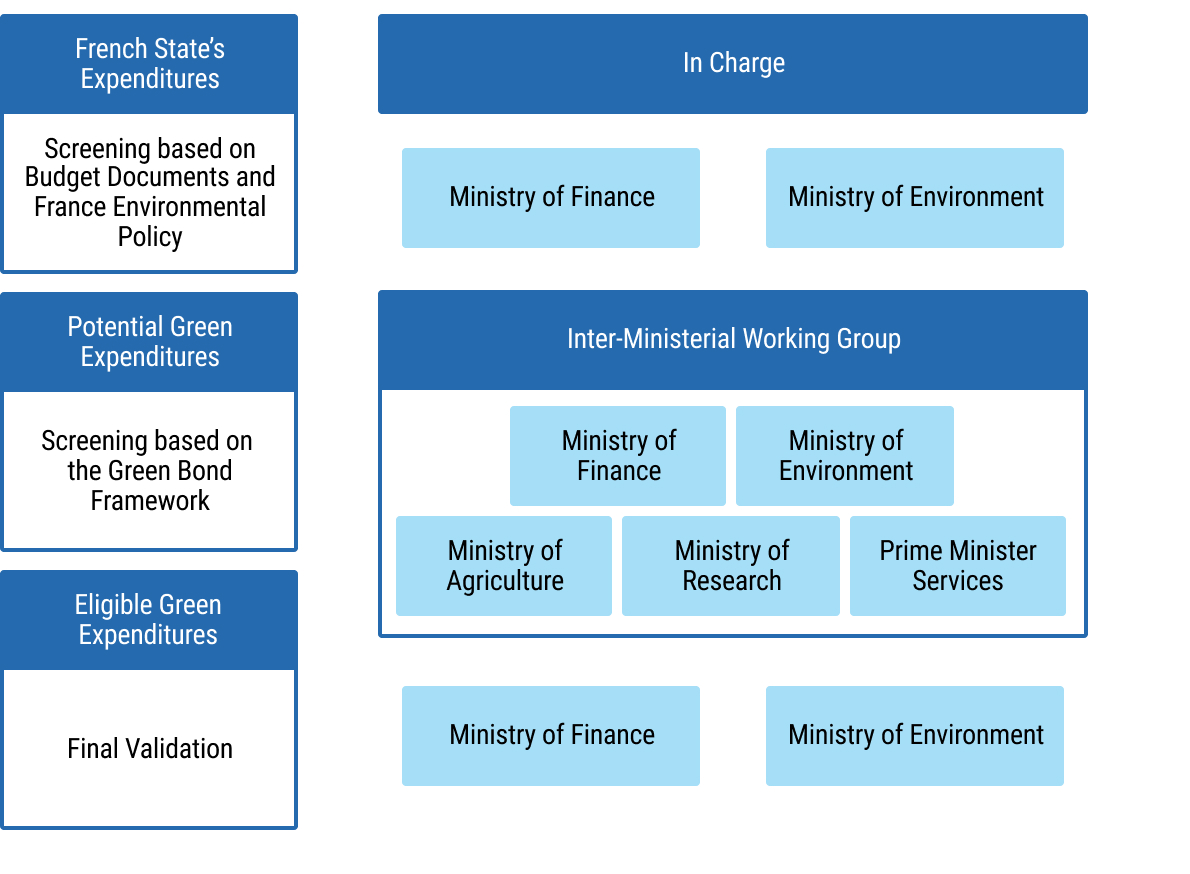 chap5_img_3 chap5_img_3 |
- chap5_ol_2
- chap5_li_26Robust monitoring, reporting and verification (MRV). Post-issuance obligations for health bonds or loans involve three main areas, which should be documented in the UoP Finance Framework:
- chap5_li_27Monitoring eligible expenditures. The MoF (typically with the Budget Directorate) tracks eligible spending in the national budget, ensuring it matches the total debt issued and is disbursed within a reasonable timeframe (usually within two to three years). To facilitate this process, expenditures and budget execution must be easily traceable in the accounting system.
- chap5_li_28Reporting to investors and the public. Annual allocation reports, which synthesise how funds were distributed throughout eligible budget expenditures, are mandatory for UoP debt instruments as per ICMA and LMA Principles. Although not compulsory, borrowers can also provide impact reports, depending on the availability of data. Reports would usually be co-drafted by the Finance and Health ministries and published on the MoF’s website.
- chap5_li_29Independent verification. Although not compulsory, it is strongly recommended to have an external third-party audit the reports to provide a limited assurance audit report. This is often a requirement by investors and lenders.
- chap5_ul_7
Sustainability-Linked Bonds and Loans for Health
Description and Rationale
36chap5_p_36SLBs and SLLs are especially suited for sovereigns in need of flexible funding, while embedding health goals. Unlike UoP debt instruments, there is no restriction on specific line-item or project spending. Instead, the country will commit to achieving pre-agreed performance targets on environmental and/or social key performance indicators (KPIs) within a specified time horizon. The cost of financing SLBs and SLLs will be tied to the borrower’s performance across these KPIs:
- chap5_ul_8
- chap5_li_30If the pre-defined performance targets are successfully met, the borrower may benefit from an interest rate step-down. This means that for the remaining duration of the instrument, the lenders will reduce the interest amounts that the borrower will need to service.
- chap5_li_31If the targets are not met, the borrower may suffer an interest rate step-up. In this case, lenders will increase the interest amounts that the borrower will need to service until the end of the instrument’s life.
37chap5_p_37The selection of the KPIs and associated performance targets (commonly referred to as sustainability performance targets (SPTs)) should reflect the borrower’s national social and/or health commitments. It will be thoroughly monitored and verified throughout the life of the SLB/SLL. As such, KPIs should be relevant, material, quantifiable and externally verifiable metrics that can be reliably benchmarked against standard-setting norms (ICMA/LMA). The associated targets should be ambitious and represent a material improvement beyond a business as usual scenario (I.e. without funding).
38chap5_p_38SPTs and KPIs also play a crucial role in securing credit enhancement from international institutions that aim to support the health sector. See Chapter 8: Credit Enhancement for more details.
Case Study: Republic of Côte d’Ivoire - Sustainability-Linked Loan Structured with the Support of the World Bank (August 2025)39chap5_p_39In August 2025, the Republic of Côte d’Ivoire issued its first EUR 433 million SLL, building on its inaugural Sustainability-Linked Finance Framework published in June 2025, with the support of the World Bank Group. 40chap5_p_40This Framework is articulated around 3 KPIs in the forestry and energy sectors. For each KPI, an SPT has been defined, to be achieved by the Republic by 2030 and which would result in interest rate changes from 2031 until the final maturity of the loan (2040). The table below summarises these KPIs and SPTs. 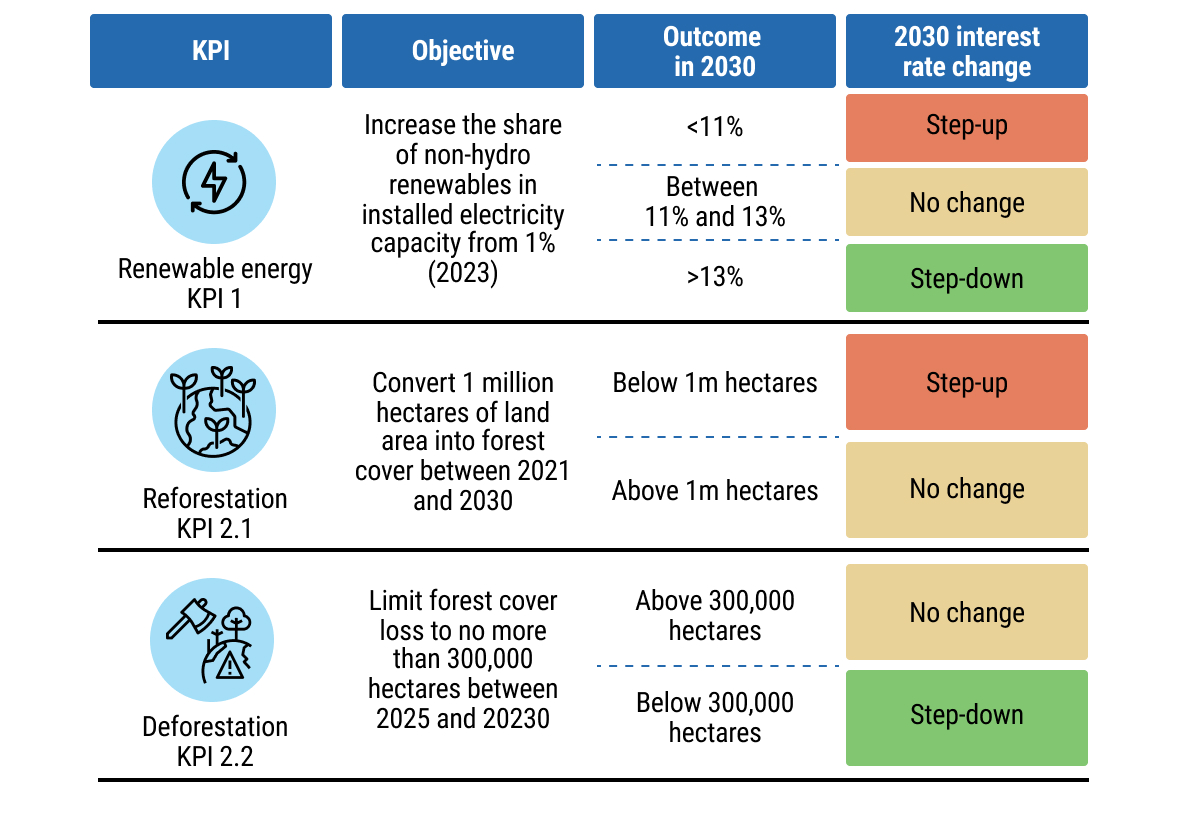 chap5_img_4 chap5_img_4 |
|
41chap5_p_41The SLL issued based on this Framework has benefited from strong support from the World Bank Group: it was the first-ever combination of two different World Bank guarantee products: (i) a Policy-Based Guarantee by the International Bank for Reconstruction and Development (IBRD), and (ii) a Non-Honouring of Sovereign Financial Obligations by the Multilateral Investment Guarantee Agency (MIGA). The graph below highlights the highly innovative structure. 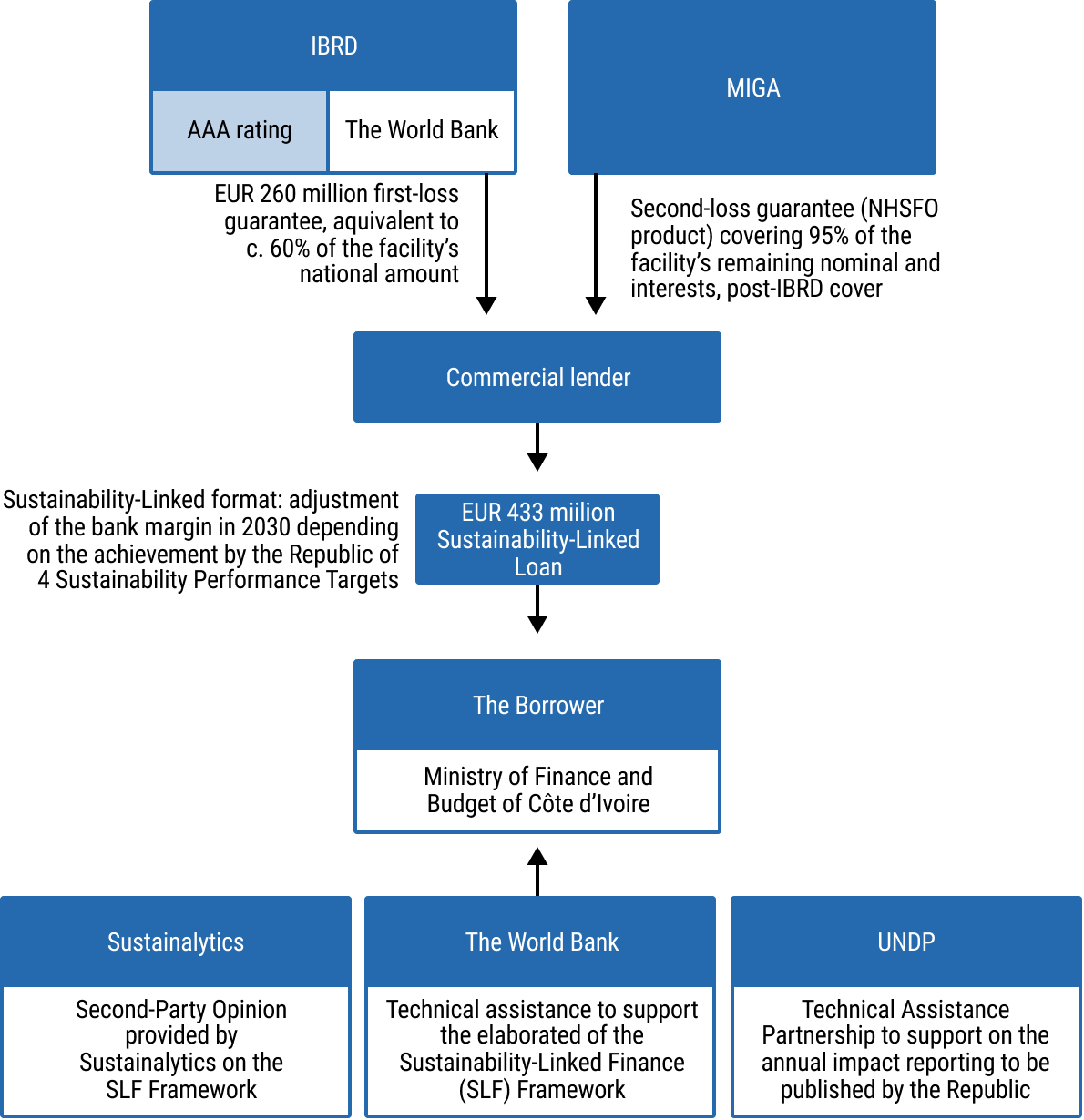 chap5_img_5 chap5_img_5 |
Enabling Conditions
42chap5_p_42Strong political buy-in. Strong political leadership is essential to ensure coordination across ministries and agencies - especially for SLBs/SLLs, which require more collaboration than UoP instruments. These instruments involve continuous monitoring of KPIs and SPTs throughout their life. The MoH must have adequate resources to meet its targets, while the MoF needs regular updates to report to investors. Identifying a political champion can help sustain this long-term effort. Leadership and ownership should ideally come from both the MoF (via the DMO or directly) and the MoH. To manage the process efficiently, establishing an interagency coordination body is recommended.
43chap5_p_43Conducive legal and regulatory frameworks. Similar to health bonds and loans described above, the borrowing country’s statutory, legal and regulatory framework must also allow for the issuance of a sustainability-linked debt instrument or be supplemented to do so. However, because SLL and SLBs do not specify the use of funds, countries should not be constrained by legal restrictions related to the earmarking of funds.
44chap5_p_44Robust data infrastructure. SLBs and SLLs require strong, reliable data that investors can trust. According to ICMA and LMA Principles, KPIs must be relevant and material to economic, social and governance policies, aligned with national sustainability priorities such as health strategies, measurable using consistent methodologies, externally verifiable and benchmarkable.
45chap5_p_45Health-related KPIs can be particularly challenging due to poor data quality, reliance on infrequent surveys, limited historical records and gaps in coverage. Some areas, like HIV/AIDS screening, are well supported by data, while others, such as non-communicable diseases, lack robust information because many cases go undetected. These gaps must be addressed to ensure transparency, verification and credible reporting. National authorities responsible for health data, such as the Statistics Office and the MoH, should regularly confirm their ability to collect and report reliable data. Ultimately, KPIs should be chosen based on the quality, availability and verifiability of the underlying data.
Opportunities and Challenges
Opportunities
46chap5_p_46Significant issuance potential: Similar to health bonds and loans, SLBs/SLLs can mobilise substantial financing volumes, particularly when structured as a bond issued on international markets.
47chap5_p_47Access to a broader pool of investors. Issuing SLBs or SLLs with health-related KPIs should expand the country’s investor base, appealing to social and ESG-focused funds and institutional investors that need to meet and report on sustainability targets. Most importantly, improvements in health not only deliver social benefits but should also support economic growth, creating an additional incentive for investors to engage with the country.
48chap5_p_48Gathering support from development finance institutions. In addition, these instruments could unlock interest from development finance institutions (DFIs), which could provide innovative credit-enhancement schemes. (See Chapter 8: Credit Enhancement). Global health institutions (GHIs) could also be engaged to provide technical assistance to MoHs in selecting their KPIs. Together, these could lower borrowing and transaction costs.
49chap5_p_49Flexible use of funds. Unlike health bonds and loans, SLBs/SLLs allow issuers to use funds for general budgetary needs while embedding agreed sustainability commitments, making them particularly attractive to sovereign borrowers balancing health goals with economic priorities. The money raised can also be used to repay pre-existing debt (e.g. but not exclusively, as part of a debt swap operation. For more information see Chapter 6: Debt-for-Health Swaps.)
50chap5_p_50Driving long-term health policy alignment. Sovereign SLLs and SLBs can be designed to drive policy change by linking borrowing costs to performance. Missing agreed targets can increase financing costs, therefore creating a strong incentive for governments to allocate sufficient resources to health. For example, a transaction could include a commitment to update a Universal Health Care law to provide free maternal health services.
Challenges
51chap5_p_51Credibility and KPI enforcement. Weak or vague health KPIs risk undermining the effectiveness of SLBs and SLLs. Ensuring that targets are material, ambitious, measurable, independently verified and aligned with ICMA or LMA Principles mitigates these concerns. Governments can seek technical assistance from GHIs or other implementation partners to strengthen their national MRV systems.
52chap5_p_52Investor awareness and market depth. The market for health-related SLBs and SLLs is still emerging, as most sustainability-linked issuances have focused on climate or nature KPIs. Building investor confidence will require transparent reporting and standardised KPI frameworks. Conducting investor soundings alongside the development of a Sustainability-Linked Finance Framework, as Côte d’Ivoire did in 2025, helps ensure that KPIs and SPTs align with market expectations. In parallel, multilateral development banks (MDBs) and other credit enhancement providers should advocate with private lenders to encourage the broader adoption of sustainability-linked instruments, including the acceptance of more meaningful interest step-downs than are currently offered.
53chap5_p_53Need for capability-building. Many sovereigns lack experience in integrating health KPIs into financial instruments and structuring adequate SLBs/SLLs. Policy and technical support, capacity building and regulatory guidance from multilateral institutions can strengthen implementation.
54chap5_p_54Complex transaction preparation. Developing an SLL/SLB framework aligned with relevant standards like ICMA or LMA takes time and coordination across key ministries (e.g. MoH, MoF). However, this framework can be reused in the future: if the government wants to issue another bond, the existing framework can be expanded to include other KPIs in the Framework (see Case Study on the example of Chile below).
Case Study: Evolution of the SLB Framework in Chile, Including Social KPIs55chap5_p_55In its initial SLB Framework, published in March 2022, Chile established two KPIs with their corresponding SPTs. 56chap5_p_56The KPIs are as follows: 57chap5_p_57KPI 1. Greenhouse gas (GHG) emissions per year, measured in metric tons of carbon dioxide equivalent. 58chap5_p_58KPI 2. Non-conventional renewable energy generation. 59chap5_p_59Later, in June 2023, considering the relevance of gender equality and social factors to the country, which were also reflected in the previous expansion of its Green Bond Framework to include social projects, a similar approach was followed in the SLB Framework, incorporating an additional KPI. 60chap5_p_60The new KPI is as follows: 61chap5_p_61KPI 3. Women’s representation on corporate boards is typically measured as a percentage of the total number of board members. |
Implementation
62chap5_p_62Issuing a sustainability-linked debt instrument will require thorough preparation and specific execution workstreams compared to conventional debt instruments. Table 5.1 below summarises a checklist of all activities that need to be conducted through the process.
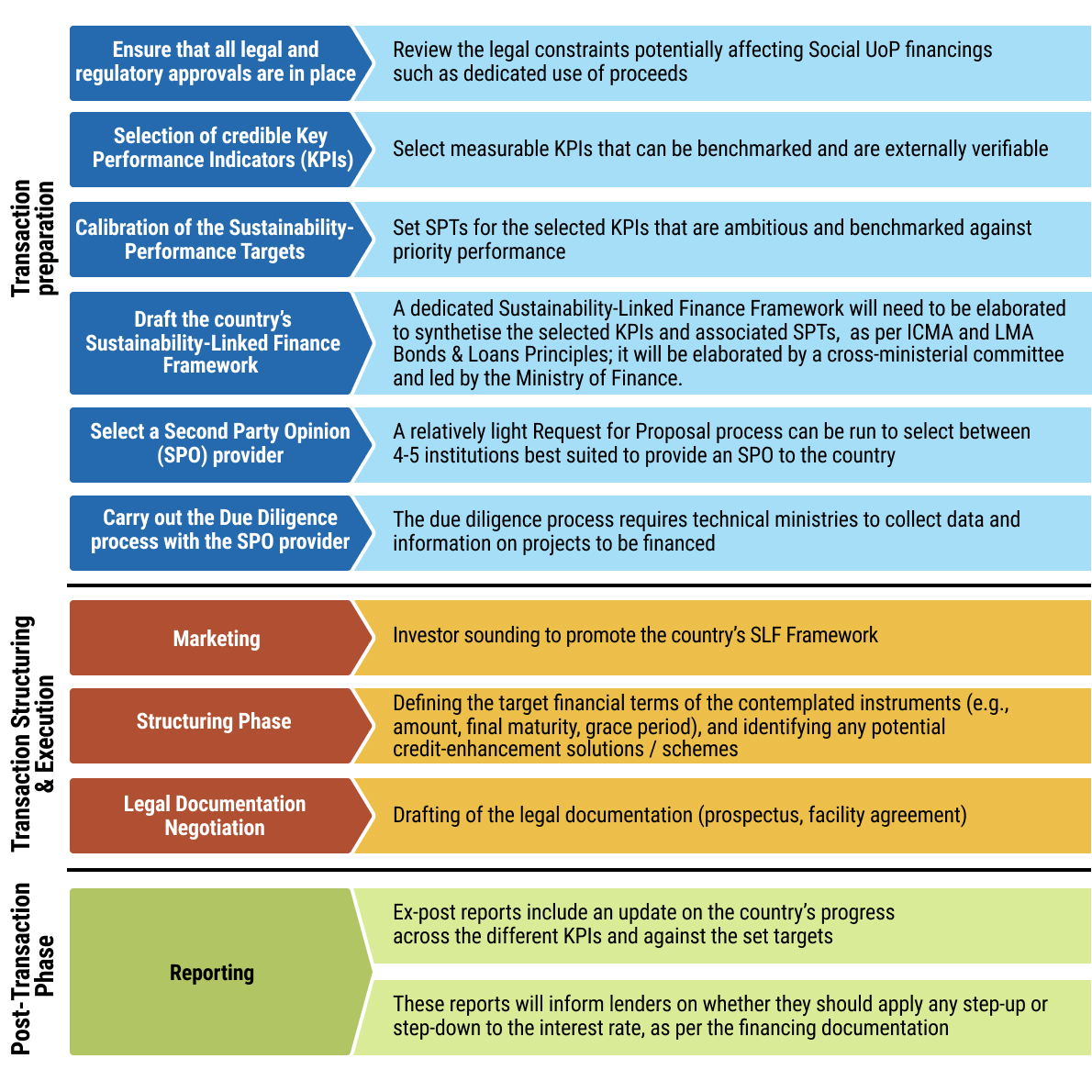 chap5_img_6
chap5_img_6
- chap5_ol_3
- chap5_li_32Preparation of a dedicated Sustainability-Linked Finance Framework. Similar to health bonds and loans, having this national framework is a mandatory requirement by ICMA and LMA for any borrower that wants to issue a sustainability-linked debt instrument on the international markets aligned with their Principles. The existence of a national strategy with clear health policy priorities will be crucial in developing the Framework, particularly in selecting KPIs and calibrating SPTs. Indicators and targets should be sufficiently ambitious to ensure the Framework’s credibility and attract investor interest, yet realistic given the country’s capacity for monitoring, reporting and verification. The MoH should play a leading role in developing any such Framework, in close collaboration with the MoF.
Case Study: Format and Content of a Sustainability-Linked Finance Framework (In Line with ICMA and LMA Principles)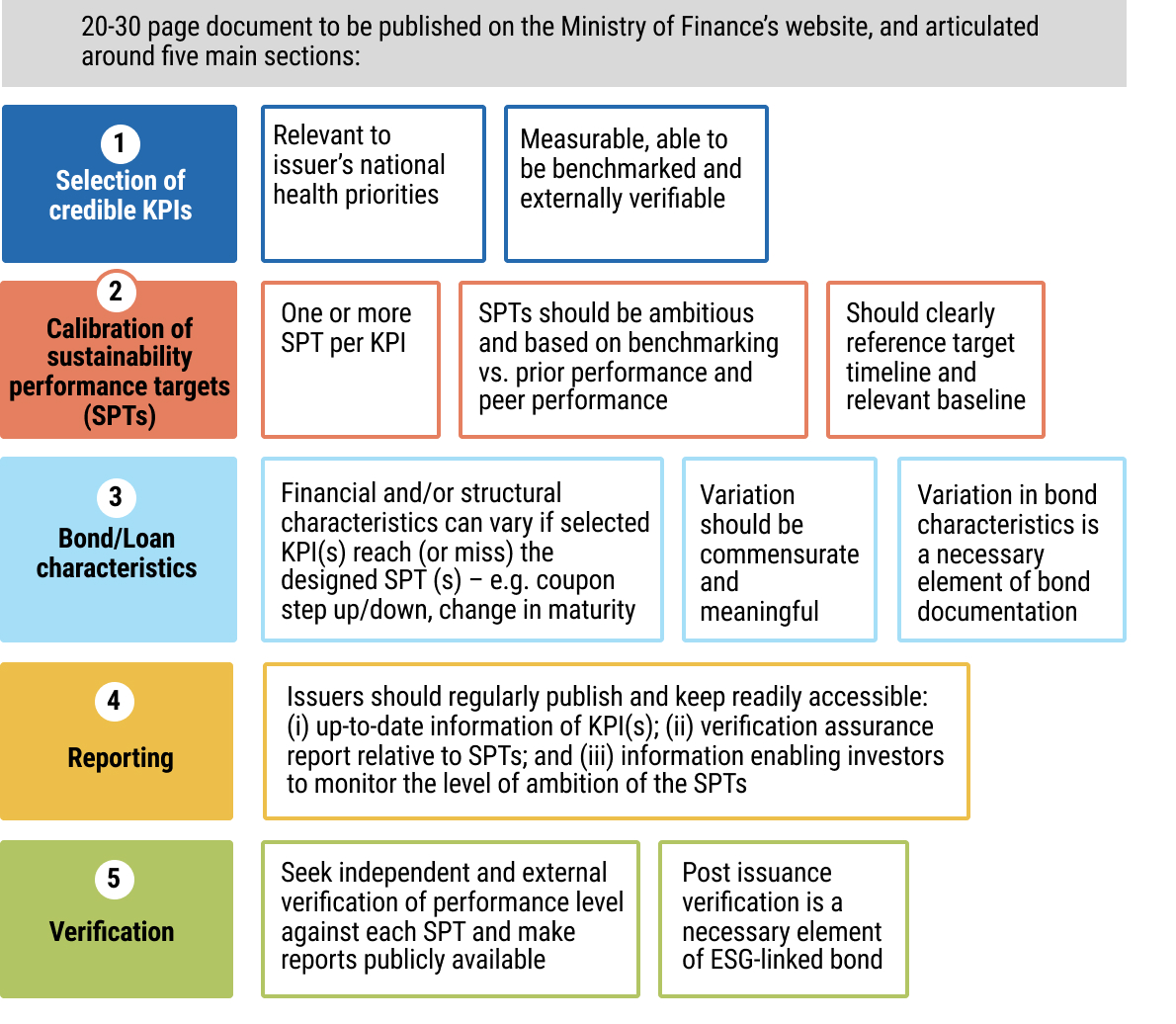 chap5_img_7 chap5_img_7 |
- chap5_ol_4
- chap5_li_33Strong stakeholder engagement. Like health bonds and loans, SLBs and SLLs require close coordination among key stakeholders. The MoF and its DMO typically lead the process, ensuring alignment with government priorities and managing structuring and negotiations with investment banks and advisors. The MoH plays a critical role in defining and selecting appropriate KPIs and targets, bringing sector expertise to the design phase and ensuring alignment with existing national health plans.
- chap5_li_34Robust financial structuring. The structure of the instrument, including the total amount, final maturity and any credit-enhancement mechanism, must be carefully aligned with the country’s debt-carrying capacity to avoid creating undue fiscal pressure. Equally important is the calibration of interest step-down and step-up mechanisms associated with the SPTs. These adjustments should be meaningful enough to incentivise governments to meet their targets and not incur additional interest payments, while remaining realistic and proportionate to the country’s fiscal capacity. Striking this balance ensures that the financial structure reinforces policy objectives without compromising debt sustainability.
- chap5_li_35Monitoring, reporting and verification. Regarding a health bond or loan, sustainability-linked instruments will require thorough annual reporting to be executed following the completion of the operation. Therefore, an effective MRV system must deliver reliable, publicly accessible and regularly updated data. It should define clear processes and transparent commitments for issuers, using trusted public databases such as those provided by the World Health Organisation (WHO) or the World Bank. This ensures investors and other stakeholders have accurate, verifiable information on the financial and structural characteristics of health SLBs and SLLs. In addition, since funding from an SLB/SLL is not explicitly earmarked for KPI achievement, it will be essential to ensure that these commitments are considered during the annual budget formulation process, allowing the MoH to implement essential activities on time and avoid potential penalties.
|
63chap5_p_63KPI policy area |
64chap5_p_64SDGs |
65chap5_p_65KPI |
66chap5_p_66Frequency: |
67chap5_p_67Data source: |
|
68chap5_p_68Communicable diseases |
69chap5_p_69SDGS 3.3: |
70chap5_p_70HIV Viral Suppression- People on HIV treatment who have suppressed viral loads 71chap5_p_71Ratio of: |
72chap5_p_72Annual |
73chap5_p_73https://indicatorregistry.unaids.org/ indicator/people-living-hiv-who-have-suppressed-viral-loads |
|
74chap5_p_74Health systems - vaccination |
75chap5_p_75SDG3:3.b Support the research and development of vaccines and medicines for the communicable and non‑communicable diseases that primarily affect developing countries, provide access to affordable essential medicines and vaccines, in accordance with the Doha Declaration on the Trade-Related Aspects Of Intellectual Property Rights Agreement and Public Health, which affirms the right of developing countries to use to the full the provisions in the Agreement on Trade-Related Aspects of Intellectual Property Rights regarding flexibilities to protect public health, and, in particular, provide access to medicines for all |
76chap5_p_76Proportion of the target population covered by all vaccines included in their national programme |
77chap5_p_77Annual |
78chap5_p_78https://unstats.un.org/sdgs/ metadata/files/Metadata-03-0b-01.pdf |
|
79chap5_p_79Maternal and child health and nutrition |
80chap5_p_80SDG 3.2 By 2030, end preventable deaths of newborns and children under 5 years of age, with all countries aiming to reduce neonatal mortality to at least as low as 12 per 1,000 live births and under‑5 mortality to at least as low as 25 per 1,000 live births |
81chap5_p_81Neonatal mortality rate |
82chap5_p_82Annual |
83chap5_p_83https://data.who.int/indicators/ i/E3CAF2B/A4C49D3 |
Impact Bonds
Description and Rationale
84chap5_p_84An impact bond is a contractual arrangement that funds a project between a government and/or donor, an investor and a service provider. The grant funder pays out only if, and only if, pre-agreed outcomes are achieved - the term “bond” is thus somewhat of a misnomer. The contracts commit the government/donor to make payments upon achievement of pre-agreed health outcomes, which the investor finances for the service providers to deliver. The donor may be a development partner or a private philanthropic organisation. Examples of impact bonds include improvements in weight gain for low-birth-weight or premature newborns, as well as a defined increase in the number of cataract surgeries and in visual acuity post-surgery.
85chap5_p_85An impact bond brings multiple parties together, each focusing on their specialisation:
- chap5_ul_9
- chap5_li_36Government and/or donor(s) who seek to maximise the benefits for target populations using scarce grant resources. They are defined as outcome funders because they pay based on the achievement of outcomes.
- chap5_li_37Socially-oriented investor(s) who seek both to have a positive social impact and a return on capital to reinvest in the future.
- chap5_li_38Service provider(s) such as a non-profit or social enterprise, which are incentivised to constantly adapt and innovate in their programmes to achieve the pre-agreed outcomes and for the maximum benefit of the populations they work with.
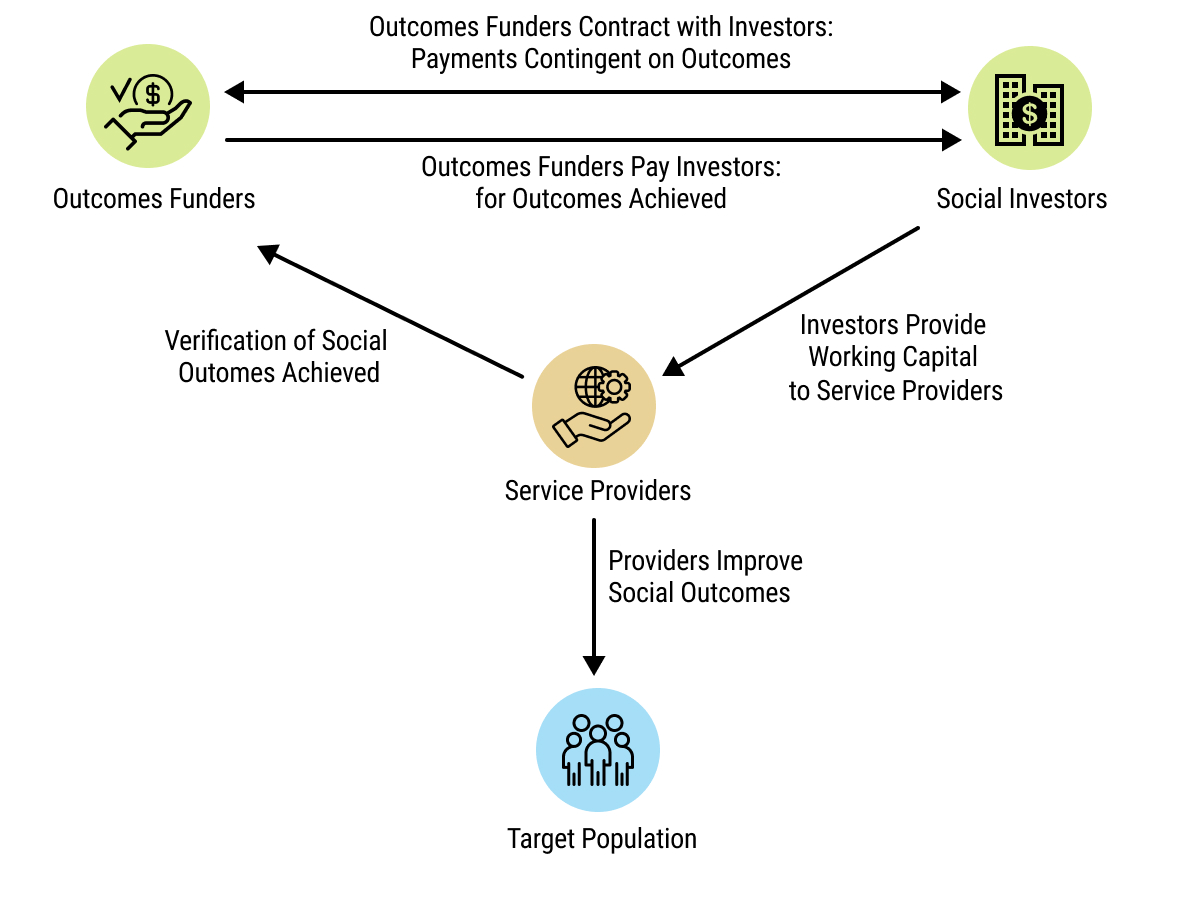 chap5_img_8
chap5_img_8
86chap5_p_86As impact bonds are typically less than USD 10 million, they are often best suited to piloting new ways of delivering health services and adding value when:
- chap5_ul_10
- chap5_li_39There is a demonstrated need for an outcome-focused approach in the specific target sector/geography.
- chap5_li_40There are promising interventions with some but incomplete evidence behind them, which could be refined through innovation and adaptation.
- chap5_li_41The chosen service providers lack access to adequate working capital or are unable to bear the risk of implementation.
87chap5_p_87Impact bonds in the health sector (follow to this link here for details) have been successfully used in Africa in:
- chap5_ul_11
- chap5_li_42Cameroon (neo-natal health; cataract surgery; hepatitis treatment)
- chap5_li_43Ethiopia (menstrual health and hygiene)
- chap5_li_44Kenya (adolescent sexual and reproductive health)
- chap5_li_45South Africa (vulnerable adolescent girls and young women)
- chap5_li_46Democratic Republic of Congo, Mali, Nigeria (physical rehabilitation)
Enabling conditions
88chap5_p_88Legal/regulatory. Impact bonds require that investors and the outcome funder establish a legal agreement (including, as needed, the establishment of a special-purpose vehicle (SPV), a temporary and ring-fenced legal entity set up for this specific purpose). Unlike the instruments described above, the government is not incurring any debt; instead, it is committing to make payments to investors upon achieving outcomes. Therefore, considerations regarding government debt issuance do not apply in this case.
89chap5_p_89Political buy-in. Ideally, outcome funding will either come from, or be channelled through, the government. This requires government buy-in notwithstanding that the government is not incurring any debt. Instead, an impact bond is beneficial to the government since it only makes outcome payments if the agreed, independently verified outcomes are achieved.
90chap5_p_90Data. Robust data at the project level are needed for the baseline against which outcomes are measured, to set ambitious yet reasonable targets, and for the outcomes themselves. This data needs to be verifiable by a third party, similar to an SLB/SLL.
Opportunities and Challenges
Opportunities
91chap5_p_91Impact bonds foster:
- chap5_ul_12
- chap5_li_47Accountability for results. Payments will not be made unless outcomes are achieved. This creates accountability for results throughout the programme.
- chap5_li_48Innovation. Service providers are only accountable for delivering outcomes, not a work plan, and can therefore adapt, innovate, and respond to evolving circumstances to achieve that. Up-front capital from the investor gives the financial space for this innovation.
- chap5_li_49Incentives to outperform. A well-designed impact bond typically features a graduated bonus for outperformance, capped at a certain level.
- chap5_li_50Cost-effectiveness. If the structuring is efficiently managed, impact bonds can improve cost-effectiveness by incentivising the maximisation of outcomes delivered per dollar.
Challenges
92chap5_p_92Impact bonds require:
- chap5_ul_13
- chap5_li_51Risk. An investor willing to take on the delivery risk (although in practice, this has often not been an obstacle given the volume of social capital available globally).
- chap5_li_52Metrics. Clear outcome metrics agreed by all parties.
- chap5_li_53Data. Availability of outcome data that can be independently verified at a reasonable cost and in a reasonable time.
- chap5_li_54Legal Structuring. A sometimes complex legal structure that may take time and legal fees to define and agree, especially for those participating in their first impact bond.
Implementation
93chap5_p_93The implementation of an impact bond is the responsibility of the investors, subject to the observance of the government’s and the outcome funder’s (if different) fiduciary, social and environmental standards. Government contractual involvement centres on a standard funding agreement with a donor (if any).
94chap5_p_94An impact bond may require an Independent Verification Agent (IVA), depending on the chosen verification approach. If outcomes can be verified using data that is already being collected, a third-party verification is not necessarily required. In particular, the following questions need to be addressed:
Questions That May Need to Be Answered During Structuring
|
Case Study: Impact bond for Kangaroo Mother Care (KMC), Cameroon95chap5_p_95Description: Tackling neonatal mortality for premature and low-birth-weight infants
96chap5_p_96The approach has been demonstrated to reduce infant mortality and morbidity significantly in low-resource contexts. 97chap5_p_97Structure: 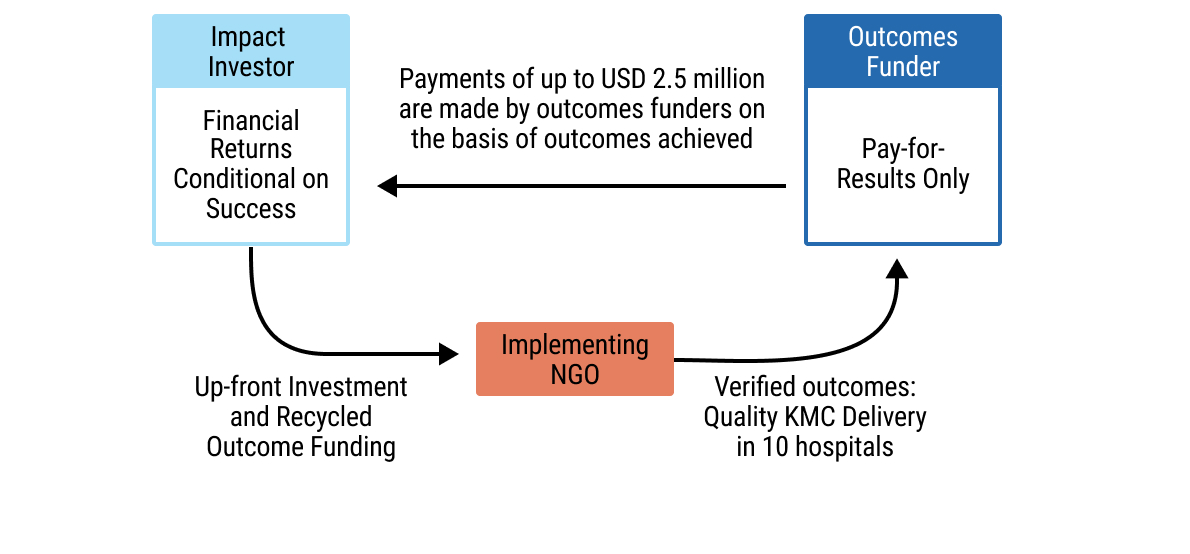 chap5_img_9 chap5_img_998chap5_p_98Objectives, Metrics and Results: The impact bond aimed to reduce mortality among premature and low-birth weight infants by scaling and improving KMC practice across Cameroon.
|
Key Legal Considerations
99chap5_p_99Understanding the legal documentation (as well as its relevant jargon) that underpins sustainable finance transactions is essential for effective transaction implementation and ensuring that terms are both fit for purpose and adequately reflect the local context.
100chap5_p_100A standard loan or bond refers to a debt instrument with conventional terms and conditions governing principal, interest, repayment and default, without any thematic or performance-linked provisions. The legal documentation for health and sustainability-linked instruments largely mirrors that of standard instruments, with modifications that align the financing with predefined performance objectives.
101chap5_p_101For health and sustainability-linked instruments, the transaction’s objectives (I.e. specifying health financing or performance-related objectives) are typically achieved through additional or revised provisions within otherwise standard documentation. As a result, these instruments are less complex to structure than debt swaps, which require multiple interlinked contracts and counterparties. Please refer to Chapter 5: Sustainable Finance Instruments> for the key legal considerations associated with debt swap transactions.
102chap5_p_102This section outlines the key clauses that are found in documentation for sustainable finance instruments. It also explains how debt documents can be enhanced to increase resiliency to potential health crises in countries through the use of debt pause clauses.
103chap5_p_103For details on the key provisions and negotiation points typically found in a standard sovereign loan agreement or bond offering document, please see the ALSF’s Loan Agreement and Bond Offering Document Commentaries.
Health Loans and Bonds: What is Unique About these Instruments?
104chap5_p_104Whether structured as a loan or a bond, a health-related financing instrument is distinguished from a standard instrument by the UoP being dedicated explicitly to health-related purposes. In the case of a health loan, the terms and conditions outlined in the loan (or “credit” or “facility”) agreement between the borrower and the lender(s) will expressly prescribe the health-related purpose of the borrowing, in line with the LMA’s Social Loan Principles (SLP) that the health investment be appropriately detailed in the documentation. Similarly, for a health bond issuance, the offering document (or prospectus) and the fiscal agency or trust deed will together outline the terms and conditions of the bonds, with a dedicated UoP specified, defining the relevant health project or programme and category of eligible expenditures set out in the agreed underlying Framework, in line with ICMA’s Social Bond Principles (SBPs). Notably, while the dedicated UoP is a defining characteristic of these instruments, failure to apply the funds in accordance with the stated health purpose does not typically constitute an event of default under the debt documentation. Instead, this is generally addressed through monitoring and reporting mechanisms.
Sustainability-Linked Instruments: What is Unique About These Instruments?
105chap5_p_105SLLs and SLBs share a common feature that distinguishes them from UoP instruments such as health loans or health bonds: the proceeds are not earmarked for specific projects or categories of expenditure. Instead, both instruments link their financial terms to the achievement of predefined SPTs measured against KPIs as described above.
106chap5_p_106In the case of an SLL, the loan agreement entered into between the sovereign and the lender(s) will include provisions that tie the interest margin to performance against the agreed SPTs, incorporating a step-up or step-down mechanism whereby the interest amounts owed increase if the SPTs are not met and decrease if they are met or exceeded. The loan documentation will also typically include a requirement for independent verification of performance, as a reporting obligation outlined in the transaction documentation, to confirm whether the relevant SPTs have been achieved for the applicable period.
107chap5_p_107The box below reflects the LMA’s draft provisions for SLLs.
Sample Step-Up/Step-Down Clause108chap5_p_108Sustainability Margin Adjustment 109chap5_p_109Subject to Clause · (Declassification Event) and the other paragraphs of this Clause, · following the receipt by the Agent of the Sustainability Compliance Certificate in respect of a SLL Reference Period in accordance with Clause · (Sustainability Compliance Certificate, Sustainability Report and Verification Report), the Margin applicable to each Loan shall be adjusted (a Sustainability Margin Adjustment) (or not adjusted, as the case may be) to the applicable rate determined using the table set out below and the number of SPTs that the Sustainability Compliance Certificate for that SLL Reference Period certifies have been met:
|
122chap5_p_122SLBs also link the bond’s financial characteristics (e.g. coupon rate or redemption premium) to the issuer’s achievement of specified SPTs, consistent with ICMA’s Sustainability-Linked Bond Principles. This will also be outlined in the bond’s documentation, like that of the SLLs.
Impact Bonds: What is Unique About These Instruments?
123chap5_p_123Impact bonds represent a distinct contractual structure from those described above. Rather than adapting a standard debt instrument, they comprise a series of contracts among governments, donors, investors and service providers, under which repayment is contingent upon the achievement of predefined social or health outcomes.
124chap5_p_124An impact bond requires the following contracts:
- chap5_ul_17
- chap5_li_67Outcomes contract, between government/other outcomes funders and investors to define the amounts to be paid against achievement of each unit of outcome (or the whole outcome if it is not divisible). A clause may be necessary to permit some payment to investors in the event of force majeure events that prevent the desired outcomes from being achieved. In some cases, the service provider may also be involved in the contracting structure, but this is unusual.
- chap5_li_68Investors and Service Providers to define programme implementation, disbursement triggers and possible bonus to service providers on achievement or over-achievement of outcomes. Experience suggests that investors will want to maintain a significant degree of flexibility in the contract to allow for learning and adaptation (feedback loops).
- chap5_li_69Government/other Outcome Funders and the IVA to define the role of, and payments, to the IVA (in some cases, an IVA may not be needed if all parties agree it is not necessary).
Pandemic or Epidemic Pause Clauses
125chap5_p_125Loan and bond documentation can also be drafted to include clauses that allow the borrower or issuer to pause repayments in the case of an exogenous health event, such as a pandemic or epidemic. These are typically structured as contingent debt service deferral clauses, which provide for a temporary standstill on principal and/or interest payments upon the occurrence of a predefined trigger event such as a declaration of a public health emergency by a recognised international body (e.g. the WHO) or a national authority. The clause typically specifies the duration of the deferral period, the conditions for resuming payments and the treatment of accrued interest during the deferral. Because they provide certainty and predictability for all parties to the debt contract, these should be beneficial for both the sovereign and its creditors.
126chap5_p_126ICMA has published a sample pandemic-related pause clause, which would tie the repayment pause to a WHO declaration of a Public Health Emergency of International Concern. This formulation provides an objective trigger linked to an authoritative international body, reducing ambiguity around when the deferral trigger can be invoked.
127chap5_p_127The following is the sample pandemic event pause clause published by ICMA. The language below can be adapted as appropriate for epidemics or other health crises that may impact a country.
Sample Pandemic Event-Related Debt Clause128chap5_p_128"Deferral Event" means the occurrence of any of the following: 129chap5_p_129(a) Pandemic Event, 130chap5_p_130(b) Other. 131chap5_p_131"Pandemic Event" means the occurrence of the following sequence of events after the Issue Date: 132chap5_p_132(a) The WHO declares a Public Health Emergency of International Concern (as defined in the International Health Regulations of the WHO) with respect to any disease that grants such disease phase 6 status, or any other categorisation as the WHO may use to describe an active ongoing pandemic from time to time (PHIO) (excluding the continuation of the COVID-19 pandemic in the form of the current variants of COVID-19 existing as of the Issue Date); 133chap5_p_133(b) The [Sovereign] or any other competent political or regulatory subdivision thereof declares a state of public health emergency with respect to any PHIO declared under (a) above; 134chap5_p_134(c) And either: 135chap5_p_135(i) The occurrence of a Real Gross Domestic Product (GDP) contraction over [two consecutive quarters], which in aggregate results in a contraction of at least [•]% of Real GDP relative to [the same two quarters in the previous fiscal year (based on estimated realised GDP at constant prices for the current year and provisional realised GDP at constant prices for the prior year], as published by [•] and reported to at least [two] of: the International Monetary Fund (IMF), the World Bank and [insert any appropriate regional MDB]); and/or 136chap5_p_136(ii) The events described in paragraphs (a) and (b) above result in the [Sovereign] approving and enacting an increase in governmental spending (that is not rescindable) (the Pandemic Increased Spending) directly relating to the relevant PHIO (and the measures taken by the [Sovereign] in response thereto) that is at least equal to USD [•]. 137chap5_p_137For the purposes of paragraph (c)(ii) above, any reduction in budgeted government spending as a result of payments due under these [terms and conditions/Conditions] being deferred as a result of a Pandemic Event occurring shall be disregarded when determining whether Pandemic Increased Spending has been approved and enacted. 138chap5_p_138"Real GDP" means the gross domestic product of [Sovereign] at constant prices as adjusted for inflation. 139chap5_p_139For the full text, please see CRDC's November (2022) notice. |
140chap5_p_140At the time of writing this User Guide, the first country known to integrate a pandemic clause into its sovereign debt documentation is Barbados, which included a trigger tied to a pandemic emergency in its debt swap in 2022 and subsequently, including in its June 2025 sovereign bonds.
Case Study: Government of Barbados - Pandemic Clause (2022)141chap5_p_141In September 2022, the Government of Barbados completed a debt conversion (refer to Chapter 5: Sustainable Finance Instruments for an overview) for marine conservation that featured the world’s first pandemic clause. This provision, added alongside a natural disaster clause, allows the Government of Barbados to defer up to two years of principal payments (approximately USD 18 million) in the event of a qualified pandemic or natural disaster. This feature was designed to make the country’s debt terms more resilient to external shocks. 142chap5_p_142This transaction was financed by Credit Suisse and the Canadian Imperial Bank of Commerce, with The Nature Conservancy as co-guarantor and conservation advisor and the Inter-American Development Bank (IDB) as co-guarantor. It helped Barbados refinance USD 150 million of its existing debt, generating an estimated USD 50 million in savings over 15 years. These funds are dedicated to marine conservation and support Barbados’s commitment to protect up to 30% of its ocean territory. 143chap5_p_143Barbados also included these clauses in its USD 500 million eurobond, marking its return to international capital markets in July 2025. 144chap5_p_144References: 145chap5_p_145https://www.insurancejournal.com/news/international/2022/09/22/686174.htm 146chap5_p_146https://www.nature.org/content/dam/tnc/nature/en/documents/TNC-Barbados-Debt-Conversion-Case-Study.pdf 147chap5_p_147https://nationnews-brb.newsmemory.com/?publink=29e7314b6_134fa25 |
148chap5_p_148Nonetheless, pandemic deferral clauses and wider debt pause clauses are gaining traction. Indeed, bilateral official lenders, MDBs, governments and investors are increasingly recognising the value of such pause or deferral mechanisms in the face of exogenous shocks that can impact countries’ liquidity and debt sustainability. These clauses should be considered as another tool in the toolbox.
The Importance of Legal and Financial Advisors
149chap5_p_149For government officials designing and negotiating health or sustainability-linked debt instruments, it is critical not to go it alone. The technical and legal complexity of these structures necessitates specialised advice. Integrating experienced legal and financial advisors into the transaction team ensures that the documentation is aligned with best practices, international standards and domestic law, and that pricing and risk allocation are appropriately calibrated. Governments should also involve their Attorney-General’s Office (or equivalent) from the outset of the transaction to ensure that any transaction is consistent with national laws and regulations, and required approvals and legal opinions can be provided. (See also above on legal and regulatory frameworks).
150chap5_p_150The ALSF is an international organisation dedicated to providing legal advice and technical assistance to African countries in the structuring and negotiation of complex commercial transactions, including those outlined in this User Guide.
151chap5_p_151For more information on how the ALSF can support you, please visit https://www.alsf.int/
Summary of Instrument Implementation Processes and Stakeholders
152chap5_p_152The three instruments outlined in this chapter each have their own specific requirements for designing, structuring and implementation, with particular input needed from each key stakeholder. There is also a difference in the expected timeframe before issuance, ranging from 6 to 12 months for an impact bond to over 18 months for an SLB/SLL.
153chap5_p_153Figure 5.5 below summarises these key activities by instrument.
154chap5_p_154Table 5.3 following outlines the specific key role of each stakeholder.
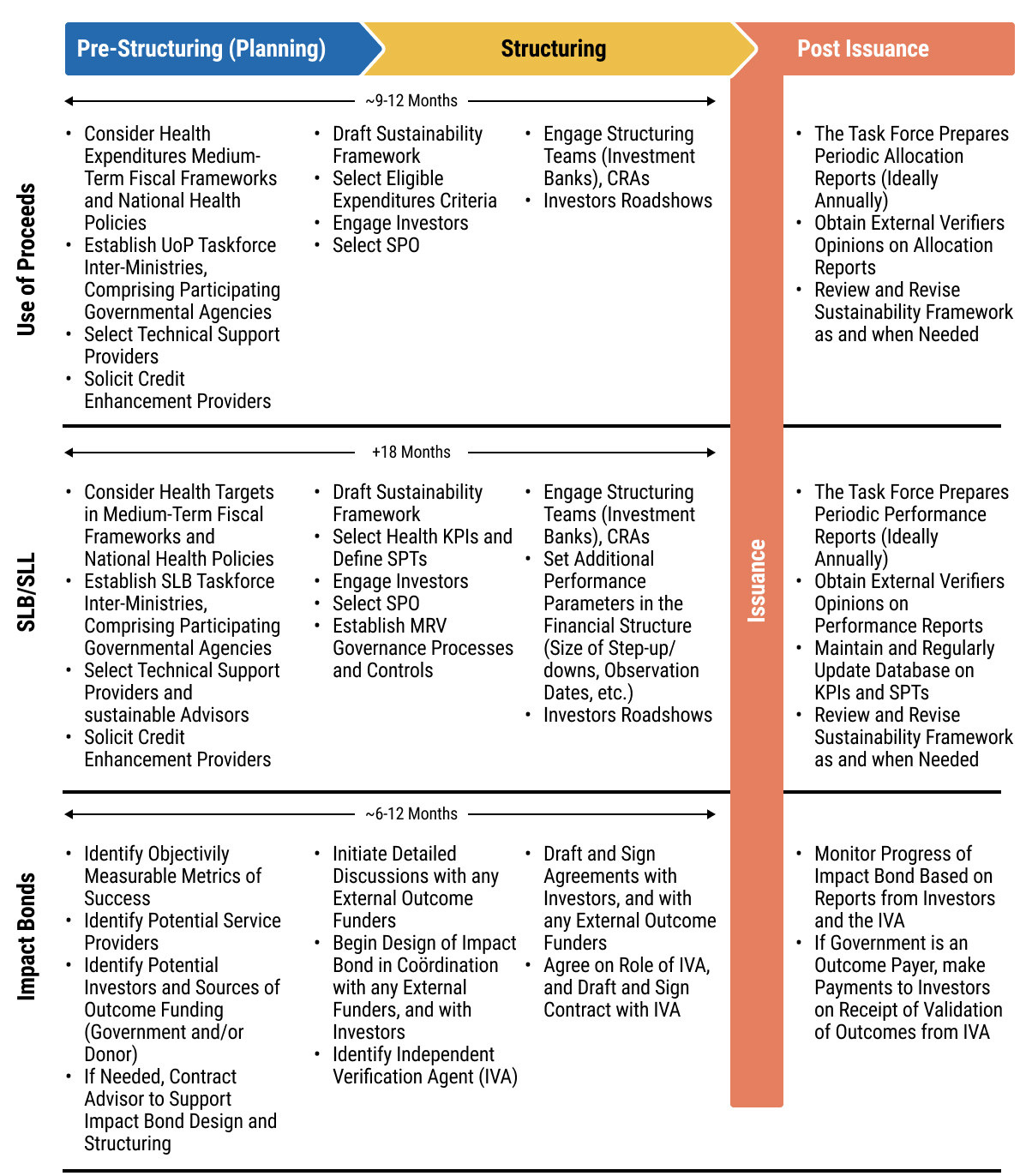 chap5_img_10
chap5_img_10
|
155chap5_p_155Stakeholder / Institution |
156chap5_p_156Core Role in UoP Bond/Loan or SLL/SLB |
157chap5_p_157Interest / Incentive |
158chap5_p_158Potential Concern / Risk |
159chap5_p_159Engagement Strategy / Framing |
160chap5_p_160Phase of Involvement |
|
161chap5_p_161Minister of Health 162chap5_p_162 163chap5_p_163Included here could be the Deputy Ministers of Health/Ministers of State for Health |
164chap5_p_164* Health bond/loan: Defines eligible health projects and investment areas. 165chap5_p_165* SLB/SLL: Identifies relevant KPIs, helps set ambitious SPTs, and develops/manages the MRV framework. 166chap5_p_166*SLB/SLL: responsible for advocating for funding needed to achieve SPT during the annual budgeting process, and ensuring strong, evidence-based implementation of the relevant activities for the selected KPI 167chap5_p_167* Both: Provides technical health input for the issuance framework. |
168chap5_p_168* Health bond/loan: Secures ring-fenced funding for specific, planned health programmes. 169chap5_p_169* SLB/SLL: Drives and demonstrates national health improvements; incentivised to meet SPTs to avoid financial penalties and gain reputational benefits. |
170chap5_p_170* Health bond/loan: Risk of funds being diverted or misallocated from intended projects. 171chap5_p_171* SLB/SLL: Risk of failing to meet SPTs, triggering financial penalties (e.g. coupon step-up) and reputational damage. |
172chap5_p_172Frame as a fiscal innovation to achieve core health mandates. 173chap5_p_173Align with the national health strategy, development plan, and debt management strategy. |
174chap5_p_174Early concept through final reporting (entire lifecycle). |
|
175chap5_p_175Minister of Finance 176chap5_p_176 177chap5_p_177Also captured here could be the Chief Economic Advisor, the Financial Secretary (Permanent Secretary for the MoF) |
178chap5_p_178Both: Custodian of sovereign debt and lead coordinator of the sustainability framework across government. 179chap5_p_179*SLB/SLL: The Budget department must ensure the KPI-related activities are budgeted and monitored during the budget cycle. |
180chap5_p_180* Health bond/loan: Secures funding for specific national priorities. 181chap5_p_181* SLB/SLL: Raises general-purpose funds while demonstrating commitment to national goals. 182chap5_p_182* Both: Diversifies the investor base; signals market leadership. |
183chap5_p_183* Dependency: Heavy reliance on other ministries (e.g. Health) for data and performance to meet reporting obligations or SPTs. 184chap5_p_184* Financial: Risk of financial penalties (step-ups) if SPTs are missed. 185chap5_p_185* Admin: High administrative burden for UoP tracking or SLB/SLL verification. |
186chap5_p_186Frame as a co-created fiscal innovation, aligning with the national debt management strategy and development plan. 187chap5_p_187Emphasise market access and investor diversification. |
188chap5_p_188Early concept through final maturity (entire lifecycle). |
|
189chap5_p_189Stakeholder / Institution |
190chap5_p_190Core Role in UoP Bond/Loan or SLL/SLB |
191chap5_p_191Interest / Incentive |
192chap5_p_192Potential Concern / Risk |
193chap5_p_193Engagement Strategy / Framing |
194chap5_p_194Phase of Involvement |
|
195chap5_p_195Presidency 196chap5_p_196 197chap5_p_197Actors here could include the Chief Minister, Minister of State, etc. |
198chap5_p_198Provides high-level political leadership, ensures cross-ministerial alignment, and sets strategic direction. |
199chap5_p_199Enhances national prestige as an innovator. 200chap5_p_200Builds credibility with international partners. 201chap5_p_201Secures a political legacy and drives national ownership of reforms. |
202chap5_p_202Competing political priorities or timelines. 203chap5_p_203Risk of reform fatigue or political opposition. 204chap5_p_204Concern over the complexity of the commitments. |
205chap5_p_205Frame as a high-visibility, legacy-defining reform. 206chap5_p_206Link to the national development agenda and international commitments (e.g. SDGs). |
207chap5_p_207Beginning (to provide mandate) and at key inflection points (to resolve bottlenecks). |
|
208chap5_p_208Parliament 209chap5_p_209Actors here could include the chairs for the parliamentary committee on health, finance, etc. |
210chap5_p_210Approves national debt operations. 211chap5_p_211Ensures accountability for public expenditure and performance commitments. |
212chap5_p_212Ensures transparency, fiscal prudence and public accountability 213chap5_p_213Gains political capital by championing innovative and effective solutions for citizens. |
214chap5_p_214Concern that the instrument is too complex or bypasses traditional oversight functions. 215chap5_p_215Political opposition or lack of cross-party support. |
216chap5_p_216Engage early with clear, non-technical briefings. 217chap5_p_217Demonstrate fiscal discipline and tangible benefits for citizens. 218chap5_p_218Identify and empower cross-party champions. |
219chap5_p_219Early consultation (pre-approval) and at key reporting/inflection points. |
Chapter 6: Debt-for-Health Swaps
Key Takeaways
|
1chap6_p_1This chapter aims to guide officials from Ministries of Finance (MoFs) and Health (MoHs), as well as practitioners, through the design and implementation of debt-for-health swaps, which provide a powerful tool to unlock fiscal savings for health objectives. The chapter emphasises that the decision to pursue a debt swap, as well as the choice of debt swap type (bilateral versus commercial, bond versus non-bond, international versus domestic), must be informed by country-specific debt profiles, fiscal objectives and health sector priorities. Each section provides a practical framework to support this decision-making process, outlining the key steps for structuring and executing successful transactions.
Fiscal Savings for Health Objectives
2chap6_p_2Debt swaps are emerging as a financial tool that can help progress towards achieving universal health coverage (UHC) in a context of narrowing fiscal space and increasing debt service pressures, through a dual impact of unlocking additional long-term health funding and reducing debt burdens. MoFs have traditionally employed debt swaps as a liability management instrument to create fiscal savings, which can be channelled to development objectives, while optimising public debt profiles, reducing refinancing risks and improving fiscal sustainability.
3chap6_p_3The traditional bilateral debt swap approach originated in the late 1980s in Latin America to support nature conservation. These transactions exchanged portions of sovereign debt for commitments to biodiversity conservation and climate resilience. Over time, other sectors have benefited from bilateral debt swaps, including health, education and food security. According to the United Nations Conference on Trade and Development, more than 230 bilateral swaps have been concluded in 58 countries since 1987, with a combined face value of nearly USD 8 billion. The Global Fund has been a major player in bilateral debt-for-health swaps, concluding 14 agreements since 2007 with an average deal size of USD 23.5 million to support national health programmes targeting human immunodeficiency virus (HIV), tuberculosis (TB) and malaria. While these operations have delivered a meaningful impact, their scale remains modest relative to the growing financing needs of health systems across Africa, primarily because they depend on the generosity of a creditor country to cancel their debt.
4chap6_p_4Since 2021, a new generation of commercial debt swaps (known as debt conversions) has emerged, significantly increasing the volume of potential transactions. It began with nature conservation in Latin America but is now being applied to a broader range of sectors, including education. This new generation of debt swaps has expanded beyond purely financial objectives to encompass structures that align debt management strategies with national development priorities. These innovative mechanisms, where a country exchanges part of its existing debt for new, guaranteed borrowing under more favourable terms, then reallocates (part of) the associated savings to specific projects, have gained traction across emerging markets as governments seek to leverage debt relief for broader socio-economic and environmental outcomes. In the environmental space, large-scale operations include transactions in Belize (2021), Barbados (2022; 2024) and Gabon (2023). Ecuador’s debt swaps in respect of the Galápagos Islands (2023) and the Amazon (2024), Bahamas (2024) and El Salvador (2024) unlocked over USD 2.1 billion for conservation, with over USD 4.6 billion of debt exchanged.
5chap6_p_5This model has also been extended to education, with Côte d’Ivoire’s (2024) transaction, which mobilised EUR 40 million for education over 5 years.
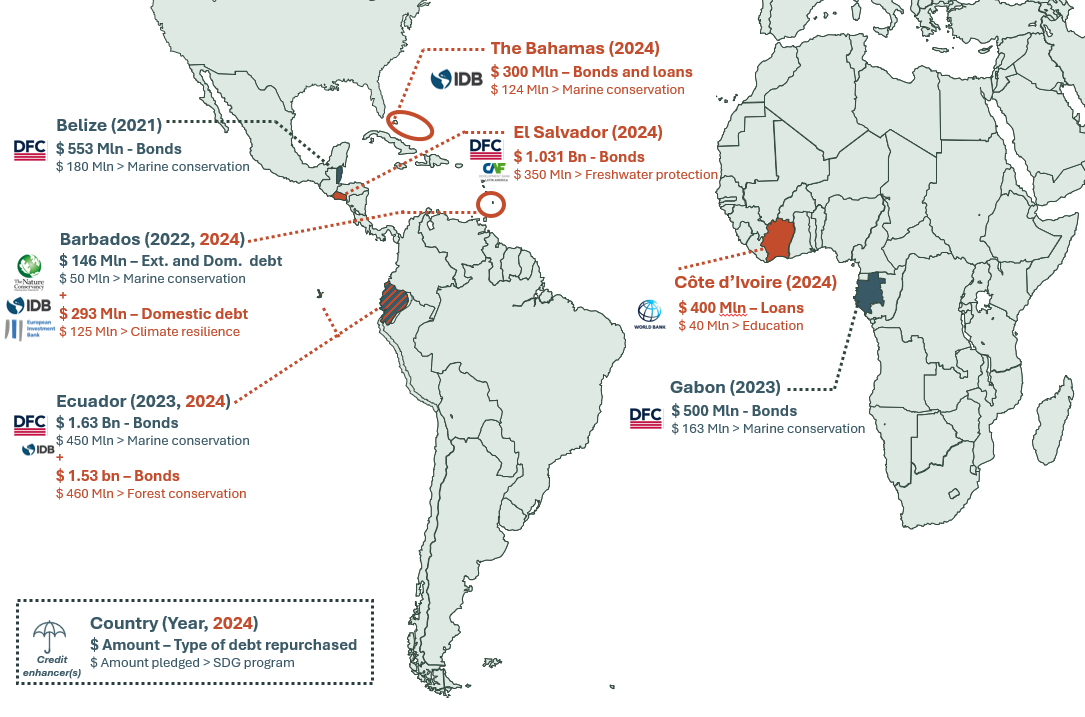 chap6_img_0
chap6_img_06chap6_p_6This context underscores the urgency of exploring debt conversions to support the health sector, through refinancing existing debt with both bond and non-bond instruments. By leveraging credit enhancement and market-based mechanisms, debt conversions could significantly amplify fiscal savings and channel resources toward health priorities at scale.
Debt Swap Structures: Bilateral versus Commercial
7chap6_p_7Bilateral debt swaps and debt conversions have distinct features. Country-specific objectives and fundamentals should guide the selection of the most suitable instrument. Table 6.1 below summarises the key characteristics of each structure.
|
8chap6_p_8Bilateral Debt Swaps |
9chap6_p_9Debt Conversions |
|
|
10chap6_p_10Debt swap mechanisms |
|
|
|
11chap6_p_11Target existing debt facilities |
|
|
|
12chap6_p_12Involved third-parties |
|
|
|
13chap6_p_13Range of debt swapped |
|
|
|
14chap6_p_14Range of programme funding |
|
|
|
15chap6_p_15Typical programme design timeline |
|
|
|
16chap6_p_16Typical financial execution timeline |
|
|
17chap6_p_17Note: The programme design phase includes agreeing on the health-linked application of freed-up fiscal savings, policy and spend commitments, as well as related monitoring and verification. The financial execution phase includes defining the structure, negotiating and executing. Depending on the situation, these two phases can be successive or run in parallel. Ranges are based on historical transactions that have been executed.
18chap6_p_18Several factors need to be evaluated to assess whether a debt swap provides the right tool in the country’s specific context. For countries facing unsustainable debt burdens, a comprehensive debt restructuring, generating substantial debt relief, is likely required. While debt swaps serve as a liability management tool, they do not address solvency issues and should be viewed as a means of providing liquidity support. The decision tree below helps to navigate the decision-making process.
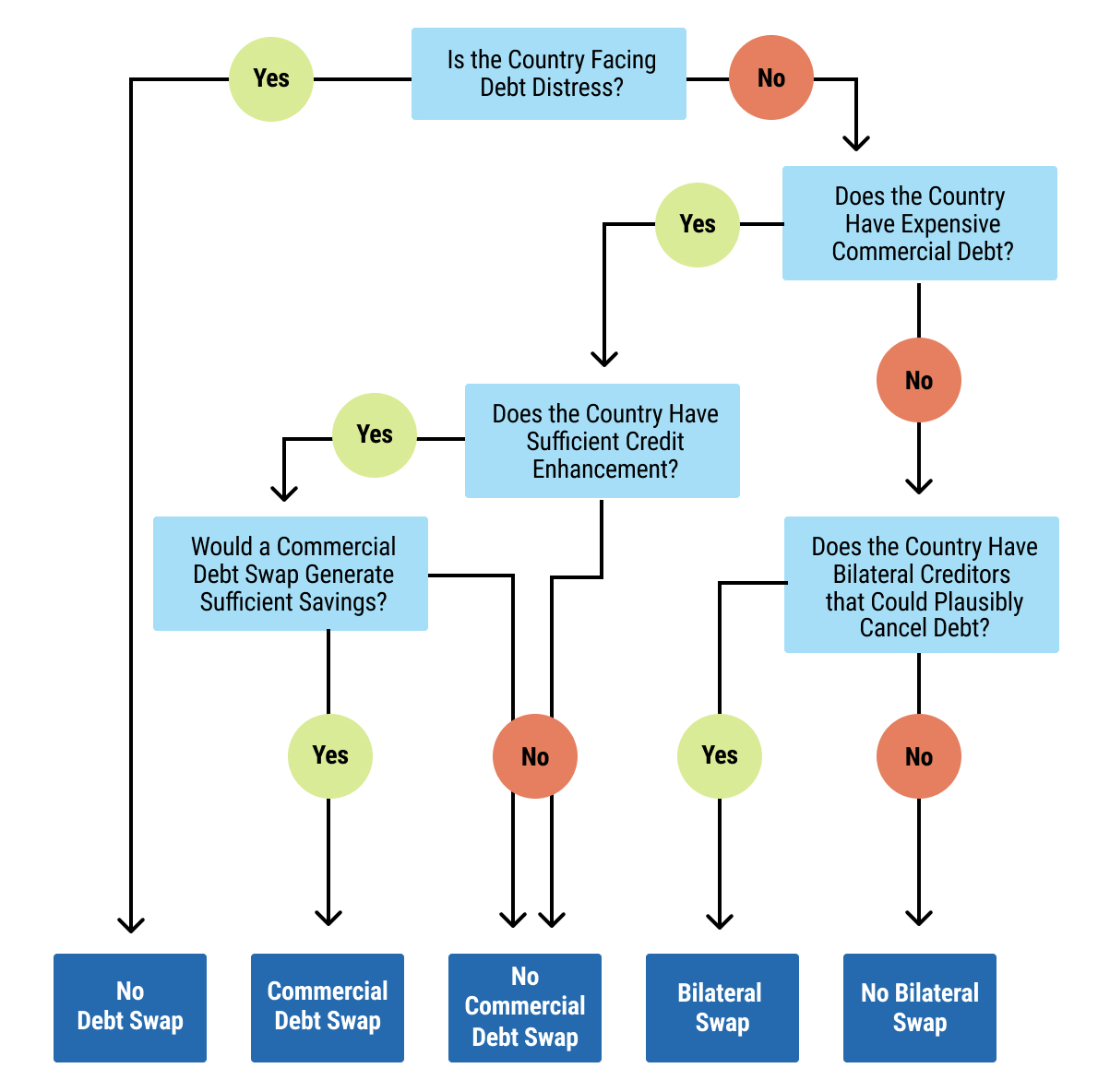 chap6_img_1
chap6_img_1Debt Swaps to Support Health Programmes
Aligning Financial Flows with Health Programmes
19chap6_p_19The financial flows generated through a debt swap are well-suited to health financing needs, as they tend to be long-term, regular and predictable. Debt swaps are not one-off grants or loans. Instead, they enable countries to redirect their savings towards long-term health objectives. When a country enters a swap arrangement, it agrees to make fixed, periodic payments into a development fund or to a specified third party, instead of paying those amounts to the original creditors. These payments are often set for the life of the swapped debt, which can be up to 20 years, as in the case of Belize, and typically above 10 years - although bilateral debt swaps can have a shorter tenure. Because they are linked to the sovereign’s debt-servicing obligations, the payment flows can become a legally binding, long-term commitment.
20chap6_p_20The unique structure of these financial flows warrants careful consideration to fully harness their potential in advancing health outcomes. Three guiding principles can help orient the nature of spending that a debt-for-health swap could support:
- chap6_ul_15
- chap6_li_26Long-term vision and government ownership. Define a clear long-term vision for what swap resources will achieve, align it with national plans, utilise consultations at both design and operational levels, and establish measurable results and outcome-based commitments to guide spending over many years.
- chap6_li_27Spending that benefits from long-term financing. Direct resources to expenditures with predictable multi-year costs or high long-term returns, for example, maintenance programmes, infectious disease surveillance systems, vaccine financing and campaigns, workforce training, climate-resilient infrastructure and broader human capital.
- chap6_li_28Additionally, with government budgets. Implement governance and selection rules that ensure swap funds do not displace baseline government spending but are instead accretive to it. Practical measures include prioritising programmes that the budget would not reliably fund, and channelling quick-release funds for emerging needs and sustained finance for longer-term programmes.
21chap6_p_21Figure 6.3 below highlights examples of health spending that could be aligned with those principles - depending on the country context.
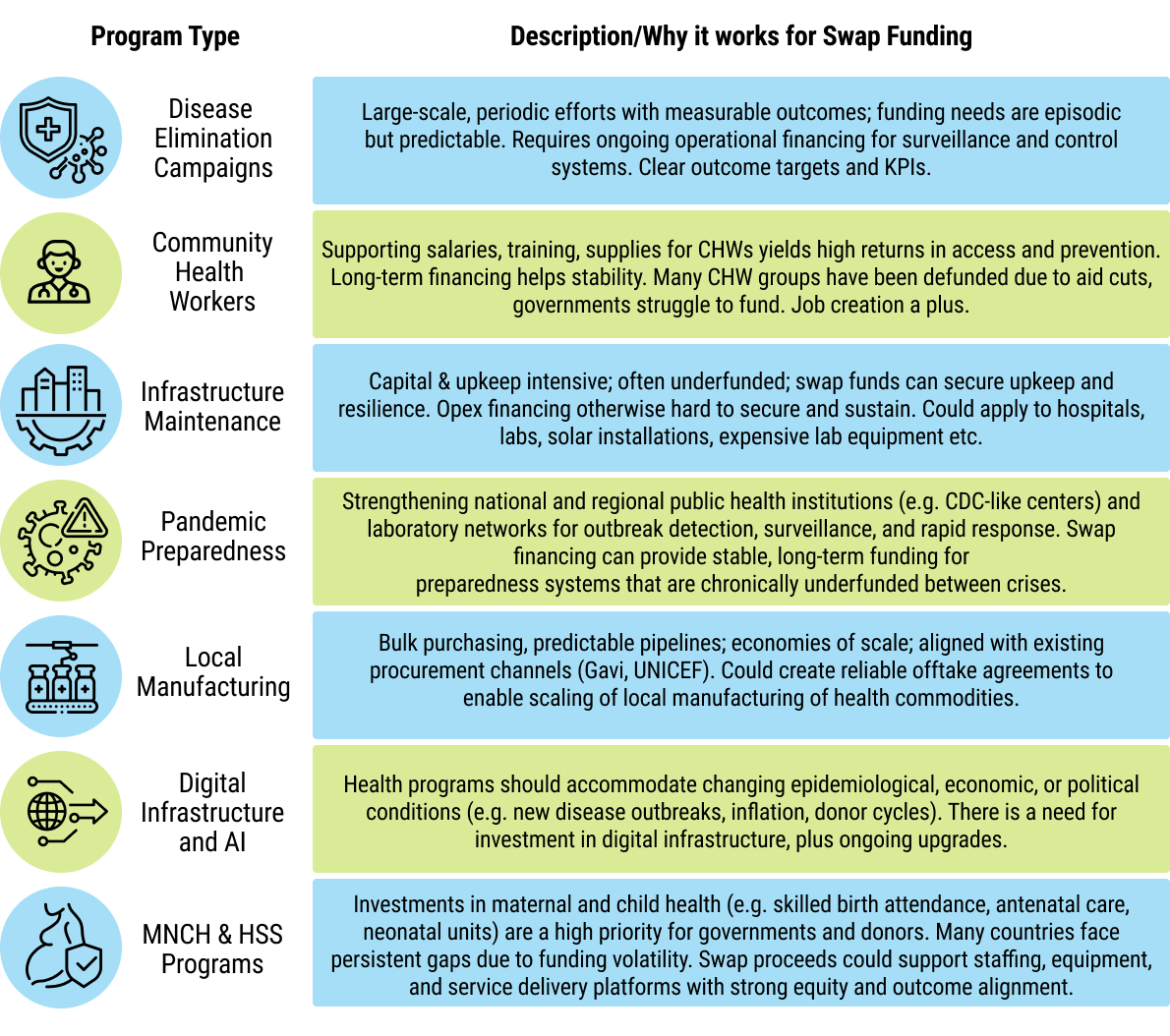 chap6_img_2
chap6_img_2
Delivering Health Programmes
22chap6_p_22Debt swap-funded programmes have traditionally been delivered by implementing entities that are accountable for the programme implementation. Often, the debt swap enabler (the bilateral creditor in a bilateral debt swap or the development finance institution providing credit enhancement in a debt conversion) requests that such intermediaries provide them with comfort regarding the programme delivery. There can be transaction costs for setting up those intermediaries, and different models have been used thus far, with costs typically going in decreasing order:
- chap6_ul_16
- chap6_li_29Setting up a dedicated trust fund. A legally independent, separate entity, with board members from the government, the implementing partner, and other independent technical experts and professionals, which ensures that the resources freed by the debt swap are applied as agreed and subject to strong governance. For example, Belize’s 2021 blue bond debt swap led to the creation of an independent conservation trust fund - the Belize Fund for a Sustainable Future (BFSF). The BFSF receives long-term payments from the Government of Belize and allocates these flows towards marine and coastal protection. It is essential to determine upfront whether a new trust fund will be used for future operations, not just the specific transaction, as this informs its design and governance, allowing transaction costs to be spread across different operations. For example, the Seychelles utilised the Seychelles Conservation and Climate Adaptation Trust, established for Seychelles’ 2015 debt swap, to receive proceeds from a blue bond transaction.
- chap6_li_30Using existing structures. Leveraging existing structures to facilitate the objectives of the debt swap, either at the national or global level.
- chap6_li_31National structures: Country-specific, national trust funds. For example, the Bahamas 2024 commercial debt swap was implemented through the Bahamas Protected Areas Fund (BPAF). The BPAF was previously established in 2014 by an Act of Parliament to provide “sustainable financing into perpetuity” for the management of the country’s protected‐areas system. The El Salvador debt swap involved a collaboration between the already existing Environmental Investment Fund of El Salvador and Catholic Relief Services.
- chap6_li_32Global structures: Instead of channelling the funds to a separate trust fund, the fiscal savings can be channelled to international organisations or development institutions already present in the country and with mandates that are aligned with the debt swap objectives. For example, the Global Fund, through its debt-for-health model, has been widely used as an implementing channel for bilateral debt-for-health swaps owing to its strong fiduciary systems, large in-country delivery footprint, and ready pipeline of technically vetted programmes that allow countries to rapidly and transparently translate debt swap proceeds into measurable health impact (see the box below: The History of Debt-for-Health Swaps).
- chap6_ul_17
- chap6_ul_18
- chap6_li_33Using country systems. For its 2024 commercial debt swap, Côte d’Ivoire is utilising its existing systems and institutions to deliver the programme. In this case, the savings are channelled into an already existing education-sector programme-for-results supported by the World Bank.
The History of Debt-for-Health Swaps23chap6_p_23Debt-for-health swaps had a brief history with the United Nations Children’s Fund (UNICEF) between 1991 and 1993, during which the institution served as the implementing organisation for seven debt-swap operations, totalling approximately USD 75 million. Older debt swaps that benefited the health sector included approximately 8% of the French add-on programme to Heavily Indebted Poor Country (HIPC) debt relief, known as the Contrat Désendettement Développement, and a debt buyback of Nigerian debt by the River Blindness Foundation to combat river blindness in 1993. 24chap6_p_24It was only after the Global Fund launched its debt-for-health programme in 2007 that debt swap resources started supporting the health sector at scale. Leveraging its role as the most prominent global health financier and its extensive operational footprint across more than 120 countries, the Global Fund introduced Debt2Health (D2H), a structured, high-integrity model that transformed debt swaps from ad hoc instruments into a reliable and scalable financing tool for health. Unlike earlier swaps, D2H embedded rigorous fiduciary oversight, transparent reporting and measurable programmatic commitments - giving creditors the assurance they needed and enabling countries to channel resources immediately into technically vetted, high-impact health interventions. 25chap6_p_25Three features of the Global Fund’s model proved catalytic. First, its existing grant architecture and trusted assurance systems (including independent audits, procurement controls and in-country grant management structures) dramatically reduced transaction costs and implementation risks. Second, its Register of Unfunded Quality Demand (UQD) (See: https://resources.theglobalfund.org/en/grant-life-cycle/grant-making/unfunded-quality-demand/) provided a ready pipeline of technically reviewed, country-owned programmes, allowing debt-swap proceeds to be rapidly absorbed without lengthy design phases. Third, the Global Fund’s established relationships with MoFs and MoHs created the political and operational alignment needed to turn cancelled debt into sustained domestic investments. 26chap6_p_26As a result, D2H became the first mechanism to deliver debt-for-health swaps at a meaningful scale, demonstrating that well-structured swaps could reliably produce additional, predictable funding for national HIV, TB, malaria and health-systems priorities - while maintaining full country ownership and alignment with national strategic plans. Between 2007 and 2025, the Global Fund closed 14 transactions involving three creditor countries (Australia, Germany and Spain), converting nearly USD 500 million of bilateral debt into USD 330 million in health funding for 11 debtor countries. Germany, in particular, contributed to more than 84% of the health investments generated by the D2H programme. |
Bilateral Debt-for-Health Swaps
Description and Rationale
27chap6_p_27Bilateral debt-for-health swaps are voluntary operations whereby a bilateral creditor agrees to cancel or reduce existing debt in exchange for a predetermined health spending commitment by the debtor country. The debtor country will reallocate all or part of the debt service on the cancelled or reduced debt to support a pre-approved health programme over time. In other words, instead of repaying the debt to the creditor, the debtor country spends it on an in-country programme. The health programme may be implemented by a reputable international organisation and/or by the government or public institutions.
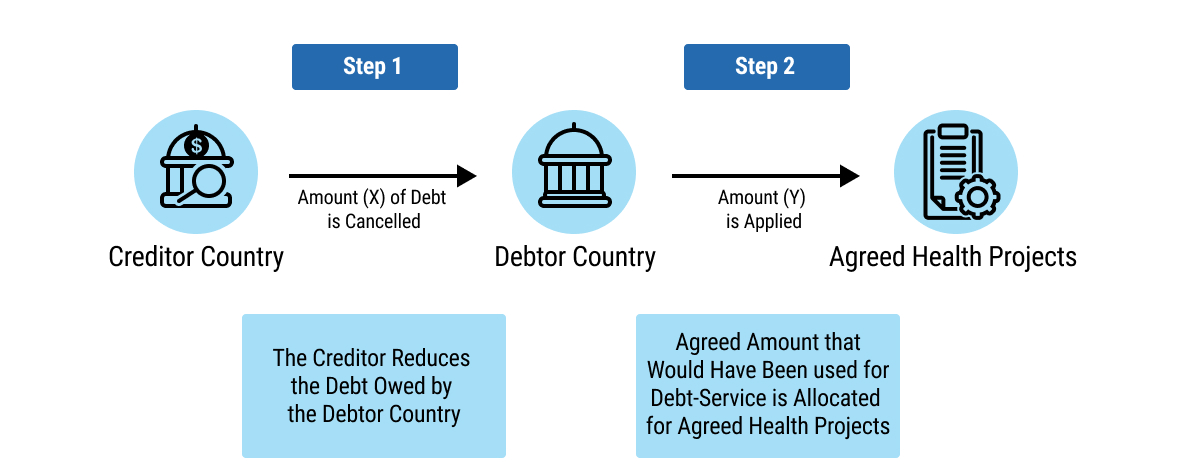 chap6_img_3
chap6_img_3
28chap6_p_28The incentives for the parties on a bilateral debt swap typically include the following:
- chap6_ul_19
- chap6_li_34For the debtor country, the transaction unlocks additional health financing while advancing national development goals.
- chap6_li_35For the creditor country, the swap provides a vehicle to reinforce its commitment to global health diplomacy, potentially increasing Official Development Assistance (ODA) under specific conditions.
- chap6_li_36For the health intermediary, it enables them to expand their operations and demonstrate a greater impact in the country.
Case Study: A Large-Scale Debt-for-Health Swap Accelerating Tuberculosis Elimination29chap6_p_29In 2022, as part of the 7th Replenishment, Germany announced a significant new commitment to the Global Fund, explicitly reaffirming that EUR 100 million of this commitment would be delivered through debt-for-health (D2H) mechanisms. Building on more than a decade of successful D2H cooperation, Germany and Indonesia initiated discussions to convert a portion of Indonesia’s bilateral debt into predictable financing for national health priorities - primarily tuberculosis (TB), a disease for which Indonesia carries the world’s second-highest burden. 30chap6_p_30The pathway from political commitment to implementation followed a structured, multi-step process:
31chap6_p_31This operation demonstrates how a clear political commitment by a creditor (Germany), strong country ownership (Indonesia) and a trusted delivery platform (the Global Fund) can turn public debt into measurable health impact at scale. It also illustrates the strengths that make the Global Fund a partner of choice for debt-for-health swaps. Through its long-standing relationships with MoFs and MoHs, the Global Fund has consistently helped align priorities between debtor and creditor countries, grounding each transaction in nationally endorsed strategies and measurable outcomes. Its established governance, fiduciary and assurance systems provide the accountability that creditors require, while dramatically reducing implementation risk and transaction costs. The Global Fund’s UQD pipeline provides a ready pool of vetted interventions, addressing capacity constraints, accelerating programme design and ensuring additionality. Moreover, by integrating swap proceeds into existing grants and national planning cycles, debt-for-health avoids parallel structures and reinforces existing systems for implementing, auditing, measuring and reporting impact. These strengths have enabled the Global Fund to deliver a series of timely, mutually beneficial debt swaps over nearly two decades, helping turn complex political and operational challenges into a durable health impact. |
Enabling Conditions
- chap6_ol_1
- chap6_li_41Identifying plausible debt for a bilateral swap
32chap6_p_32A first step is to identify the list of potential bilateral creditors. The exercise can involve compiling a list of bilateral creditor countries, including the respective size of their claims and the remaining duration, as well as whether the debt was provided based on concessional official development assistance (ODA) loans. In addition to the country’s internal debt management database, this information can also be found in public databases such as the World Bank International Debt Statistics. It would be essential to focus on the size and terms of the debt, prioritising creditors with outstanding amounts in line with the country’s health programme’s financing needs and potentially the more expensive bilateral debt.
33chap6_p_33The second step is to identify, among the existing creditor countries, those who would most likely support a debt swap. That identification exercise depends on a spectrum of indicators, including:
- chap6_ul_20
- chap6_li_42Creditor countries that have a strong bilateral relationship with the debtor country. In close collaboration with the Foreign Ministry, the debtor country can identify key creditors most likely to provide financial support, particularly for its health system.
- chap6_li_43Creditor countries that have a track record of supporting debt swaps, especially in health. Historically, Germany and Spain are the two countries that have supported the most debt-for-health swaps.
- chap6_li_44Creditor countries that have recently announced debt swap programmes.
- chap6_li_45Spain announced at the Fourth International Conference on Financing for Development in July 2025 that it would step up its debt-for-development swap efforts.
- chap6_li_46In June 2025, Italy announced a EUR 235 million debt swap programme to support local development projects over 10 years.
- chap6_li_47In July 2025, China and Egypt signed a framework agreement for the first phase of a debt swap programme through China International Development Cooperation Agency loans, marking the first such initiative by China, which may pave the way for additional debt swaps.
- chap6_ul_21
- chap6_ol_2
- chap6_li_48Political and institutional arrangements in the debtor country
34chap6_p_34Countries considering a debt-for-health-swap can leverage lessons learned from previous cases to identify the leading enablers for global implementation:
- chap6_ul_22
- chap6_li_49Strong political leadership and buy-in signal that the instrument is accepted at the political level, and therefore, that the government will be willing to invest political capital in championing the full implementation of the swap and ensuring accountability.
- chap6_li_50A clear institutional structure that defines the lead ministry, supported by other relevant ministries, departments and agencies (MDAs). The lead ministry is typically the MoF, supported by the MoH, which leads the implementation of the agreement once finalised.
- chap6_li_51Alignment with national development goals is crucial to ensure that the swap proceeds complement the government’s plans and priorities and do not establish a separate and potentially fragmented set of priorities.
- chap6_li_52Building country ownership from the start is essential to ensure transparency, accountability and the use of country systems to deliver on the debt swap, aligning with the principles of aid effectiveness and the Lusaka agenda.
- chap6_li_53The formation of an oversight and coordinating mechanism ensures that all relevant stakeholders have an opportunity to weigh in and are part of the decision-making process.
- chap6_ol_3
- chap6_li_54Early political buy-in
35chap6_p_35A debt-for-health swap involves multiple actors with distinct roles, so securing early political buy-in from a small group of high-level stakeholders is essential. These individuals will vary by country, but their endorsement signals government commitment and alignment around the process. Early engagement should be interactive and tailored, framing the debt swap in terms of each stakeholder’s priorities, pain points and incentives. To do this effectively, their internal concerns must be well understood in advance, anticipated and directly addressed in the briefing materials prepared for these discussions.
36chap6_p_36For further details on the different stakeholders involved, please see the Implementation section which follows.
Opportunities and Challenges
Opportunities
37chap6_p_37Bilateral debt swaps can mobilise additional funding for health services that align with national health strategies. This should be the starting point for a debt-for-health swap, and the government should play a key role in identifying potential uses of the proceeds. The MoH can identify health programmes that are more likely to be additional and that will not come at the expense of budget allocations from the MoF.
38chap6_p_38A bilateral debt swap can also come with additional financial benefits.
- chap6_ul_23
- chap6_li_55A bilateral debt swap might free up additional fiscal space through debt relief, which was the case in 8 of the 14 swaps implemented by the Global Fund.
- chap6_li_56Additionally, debt swaps should lower demand on foreign reserves because they typically allow the debtor country to make the repurposed payments in local currency.
- chap6_li_57Lastly, rating agencies should view bilateral debt swaps as positive even if they have typically represented only a marginal portion of the debtor country’s total debt. Given the involvement of official bilateral partners and the smaller size of the debt swaps, credit rating considerations carry less weight for bilateral debt swaps compared to debt conversions.
39chap6_p_39Working through a global health institution, such as the Global Fund, has significant upsides. The institution ensures that funding flows to pre-defined funding gaps that the government vets for their quality. In addition, its platform sets standards for transparency, inclusion, country ownership, accountability and measurable outcomes based on indicators that are independent, transparent and accurate and that involve civil society. While debt swap negotiations timelines can be protracted, the institution should have the advantage of having a pipeline of health programmes awaiting funding, for example, through its Register of UQD in the case of the Global Fund. Lastly, funds generated by debt swaps can serve as the country’s co-financing payment. This helps explain why all the identified debt-for-health swaps since 2007 have been channelled through the Global Fund.
Challenges
40chap6_p_40The primary challenge of a bilateral debt swap is aligning the incentives between the creditor and debtor countries. This involves identifying the appropriate health activity supported by the swap, as well as the implementing agency that will provide comfort to both countries. Moreover, convincing the creditor country to cancel or reduce its debt claims demands substantial negotiation.
41chap6_p_41Identifying an organisation that will be the custodian of the fiscal savings released by the debt swap and help to implement the debt swap is a key parameter in the negotiation. This organisation needs to have credibility for the implementation, monitoring and evaluation of health programmes in the country. As mentioned above, a new entity could be established, or an existing organisation identified.
Implementation
Life Cycle of a Bilateral Debt Swap
 chap6_img_4
chap6_img_4- chap6_ol_4
- chap6_li_58Identification and political agreement. Both creditor and debtor governments agree in principle on converting part, or all, of the outstanding debt into health-related funding. They assess feasibility, alignment with health and development objectives and mutual interest.
- chap6_li_59Negotiation and legal framework. A formal agreement defines the debt amount and associated treatment, including the share to be cancelled or reduced, the application of the savings generated towards an agreed domestic investment, the implementing agency and the governance structure.
- chap6_li_60Debt cancellation. The creditor cancels all, or a portion, of the agreed debt, while the debtor commits the pre-agreed payments to a national or dedicated fund, if needed, for the agreed-upon projects or programmes.
- chap6_li_61Project selection and implementation. Funds are allocated to vetted programmes aligned with national priorities and implemented through established systems or a dedicated fund.
- chap6_li_62Monitoring and reporting. Performance is tracked and reported transparently to all parties, ensuring accountability and measurable impact.
- chap6_li_63Closure and evaluation. Upon completion, results are evaluated, lessons are documented and the agreement is formally closed.
Stakeholder Engagement
42chap6_p_42Once the decision to swap debt for health has been made, the lead ministry identifies all critical stakeholders from relevant MDAs and incorporates them into the process. Involved stakeholders should be adapted to each country’s institutional and political context.
43chap6_p_43In many cases, the initiators of bilateral debt swaps are the MoF or the creditor nation. The role of the MoH in these situations is to be responsive to requests for information on priority interventions and their costs, and ensure follow-up with the MoF, leading the transaction.
44chap6_p_44That said, the MoH could be the originator of the idea of the debt-for-health swaps. In this instance, the MoH carries greater responsibility for early-stage preparation, including ensuring that the proposal is technically sound, supported by credible data, and clearly articulates the rationale for why such a mechanism is needed and how funds would be effectively utilised. If the MoF has previously raised concerns, for example, about absorptive capacity or financial management, these should be proactively addressed in an initial briefing note or concept note shared with the MoF and other high-level stakeholders. Clear, evidence-based communication at this stage builds confidence. It facilitates cross-ministerial alignment once the MoF aligns with the plan and becomes the lead for the debt swap. The MoH’s role then shifts to follow up and continued engagement in proposal writing, creditor engagements and implementation plans.
|
45chap6_p_45Stakeholder / Institution |
46chap6_p_46Core Role in Debt Swap Process |
47chap6_p_47Interest / Incentive |
48chap6_p_48Potential Concern / Risk |
49chap6_p_49Engagement Strategy / Framing |
50chap6_p_50Phase of Involvement |
|
51chap6_p_51Minister of Health 52chap6_p_52 53chap6_p_53Deputy Ministers of Health/Ministers of State for Health |
54chap6_p_54Sector policy leader; defines investment priorities and measurable outcomes for the fiscal savings generated by the debt swap; Could be the originator of the swap idea |
55chap6_p_55Stable, predictable funding for planned healthcare interventions and programmes; alignment with Sustainable Development Goal (SDG) and Universal Health Coverage (UHC) goals |
56chap6_p_56Concern that resources may not materialise or that MoF may redirect the fiscal savings generated by the debt swap elsewhere |
57chap6_p_57Frame as debt and fiscal innovation and point to alignment with national documents (national development strategy/plan, debt management strategy) |
58chap6_p_58From the early concept to the end |
|
59chap6_p_59Minister of Finance 60chap6_p_60 61chap6_p_61Debt Management Official (DMO); the Financial Secretary (Permanent Secretary for the MoF) |
62chap6_p_62Custodian of debt; face of external transactions; engages with the creditor |
63chap6_p_63Fiscal space creation; Debt sustainability; demonstration of fiscal innovation and credibility with partners |
64chap6_p_64Concern about losing control of the debt policy; concern about transaction complexity; scepticism about sector-driven proposals; concerns about absorptive capacity |
65chap6_p_65Frame as co-created fiscal innovation for health; point to alignment with health financing strategy; identify unfunded health programmes |
66chap6_p_66From the early concept to the end |
|
67chap6_p_67Creditor Country / Institution |
68chap6_p_68Counterparty to the swap |
69chap6_p_69Diplomatic and ESG visibility |
70chap6_p_70Fiduciary or reputational risk |
71chap6_p_71Emphasise transparency, accountability and co-benefits |
72chap6_p_72From the initial engagement until the end |
|
73chap6_p_73Health Development Partners |
74chap6_p_74Technical and policy support |
75chap6_p_75Programme success, portfolio impact |
76chap6_p_76Fragmentation or overlap |
77chap6_p_77Promote joint planning and unified messaging |
78chap6_p_78Feasibility → Agreement |
|
79chap6_p_79Other relevant stakeholders |
|||||
|
80chap6_p_80Presidency 81chap6_p_81Actors here could include the Chief Minister, Minister of State, etc. |
82chap6_p_82Provides political leadership, cross-ministerial alignment and strategic direction |
83chap6_p_83Mobilising funding for strategic priorities; country being seen as a leader in reforms/innovations and credibility in the comity of nations; political legacy; national ownership |
84chap6_p_84Concern about timing of reform; competing political interests |
85chap6_p_85Frame the high visibility reform potential; links to the national development agenda and regional goals |
86chap6_p_86From the beginning and at inflexion points in the process |
|
87chap6_p_87Parliament 88chap6_p_88Actors here could include the chairs for the parliamentary committee on health, finance, etc. |
89chap6_p_89Approves debt operations and ensures accountability for public expenditure |
90chap6_p_90Transparency; fiscal prudence; public accountability; positive political capital from supporting innovative solutions |
91chap6_p_91Concern about their oversight function being overruled |
92chap6_p_92Engage early with non-technical and practical briefings; demonstrate discipline and tangible citizen benefit; identify cross-party champions |
93chap6_p_93From the beginning and at inflexion points in the process |
94chap6_p_94
|
95chap6_p_95Other relevant stakeholders |
|||||
|
98chap6_p_98Attorney General / Ministry of Justice |
99chap6_p_99Legal review, compliance, approvals and provision of legal opinions |
100chap6_p_100Safeguarding sovereign integrity, ensuring due process |
101chap6_p_101Concern over liability or precedent |
102chap6_p_102Engage early; emphasise role as guardian of national interest |
103chap6_p_103From the negotiation until the agreement is signed |
|
104chap6_p_104Ministry of Foreign Affairs |
105chap6_p_105Manage the diplomatic relationship with the creditor nation; ensure alignment with foreign policy objectives; facilitate communication through official diplomatic channels |
106chap6_p_106Maintain and strengthen the integrity of the diplomatic relationship and international credibility; advance the country’s image as a reform-oriented and responsible partner |
107chap6_p_107Concern about frayed relationships if swaps don’t work out; risk of being bypassed in technical discussions |
108chap6_p_108Engage early; emphasise their role as custodians of the diplomatic relationship |
109chap6_p_109From early on in the process until the implementation |
|
110chap6_p_110Central Bank |
111chap6_p_111Foreign exchange and payment management |
112chap6_p_112Accuracy, compliance, reporting integrity |
113chap6_p_113Transaction complexity |
114chap6_p_114Involved as a technical assurance partner |
115chap6_p_115Negotiation until the implementation |
|
116chap6_p_116Health regulatory agencies |
117chap6_p_117Provide technical oversight, quality assurance and regulatory approvals for interventions funded through the swap, such as procurement of medicines, construction of health facilities or deployment of digital health tools |
118chap6_p_118Ensuring that swap-funded programmes meet national quality, safety and ethical standards; an opportunity to strengthen institutional visibility and capacity through well-managed projects 119chap6_p_119 |
120chap6_p_120Insufficient consultation leading to delays in approvals or non-compliance with national standards; risk of being perceived as bypassed in implementation oversight |
121chap6_p_121Co-opt regulators early based on the nature of funded interventions; frame participation as safeguarding quality and ensuring accountability of public investments; use them as technical verifiers or members of project review committees |
122chap6_p_122Feasibility → Implementation → Monitoring |
|
123chap6_p_123Civil Society / Academia / Media |
124chap6_p_124Oversight, communication, public trust |
125chap6_p_125Accountability, participation |
126chap6_p_126Limited access to information |
127chap6_p_127Share regular updates and accessible data |
128chap6_p_128Implementation → Monitoring |
Reporting
130chap6_p_130Transparency regarding monitoring, reporting and accountability is an essential element in the implementation of a debt-for-health swap, both for debtor and creditor countries. The reporting costs can vary significantly depending on the level of information required and when it is needed. Organisations that already have existing systems set up are likely to provide more credible reporting at a lower cost.
Debt Conversions
Description and Rationale
131chap6_p_131Commercial debt swaps are referred to as debt conversions. They are a type of liability management operation that allows a sovereign nation to replace its existing private-sector debt (such as bonds or loans) with new instruments under more favourable terms. The central purpose of this refinancing is to generate fiscal savings, which are then contractually allocated to fund specific national priorities, specifically healthcare.
132chap6_p_132Unlike bilateral swaps, which restructure government-to-government loans, debt conversions are implemented through the capital markets or banking sector, where the sovereign refinances debt held by private sector investors or lenders using proceeds from new debt (“New Debt”) to finance the buyback of the old debt. These transactions are structured around three key features:
- chap6_ol_5
- chap6_li_64Credit enhancement. The New Debt is typically credit-enhanced through guarantees or insurance from MDBs, development finance institutions (DFIs) or private sector parties (e.g. insurers or guarantors). This enhancement reduces the risk for new investors, enabling the government to secure lower all-inclusive borrowing costs (e.g. reduced interest rates) and more favourable repayment terms (e.g. longer repayment periods), resulting in financial savings (see Chapter 8: Credit Enhancement.)
- chap6_li_65Performance-linked objectives. To ensure alignment of the new financing to desirable health objectives, the New Debt is tied to legally binding policy commitments or key performance indicators (KPIs).
- chap6_li_66Governance system. A robust and accountable mechanism is utilised to manage and deploy the savings generated by the operation into the designated development objective. These can be channelled through a dedicated trust fund, through existing multilateral organisations’ programmes or through domestic government systems with equivalent oversight.
133chap6_p_133Ultimately, debt conversions can be a powerful tool for governments to create significant funding for national priorities without increasing their overall debt burdens - and often by reducing them (if the debt being repurchased, for example, trades at a considerable discount). They work by reducing fiscal expenditure on debt servicing and reallocating a portion of those savings toward financing gaps that require consistent, predictable and long-term investment. This approach can also provide a stable, long-term financing source for sovereigns that typically face costly or limited access to capital markets, offering them access to a new investor base due to their creditworthiness and pro-development features.
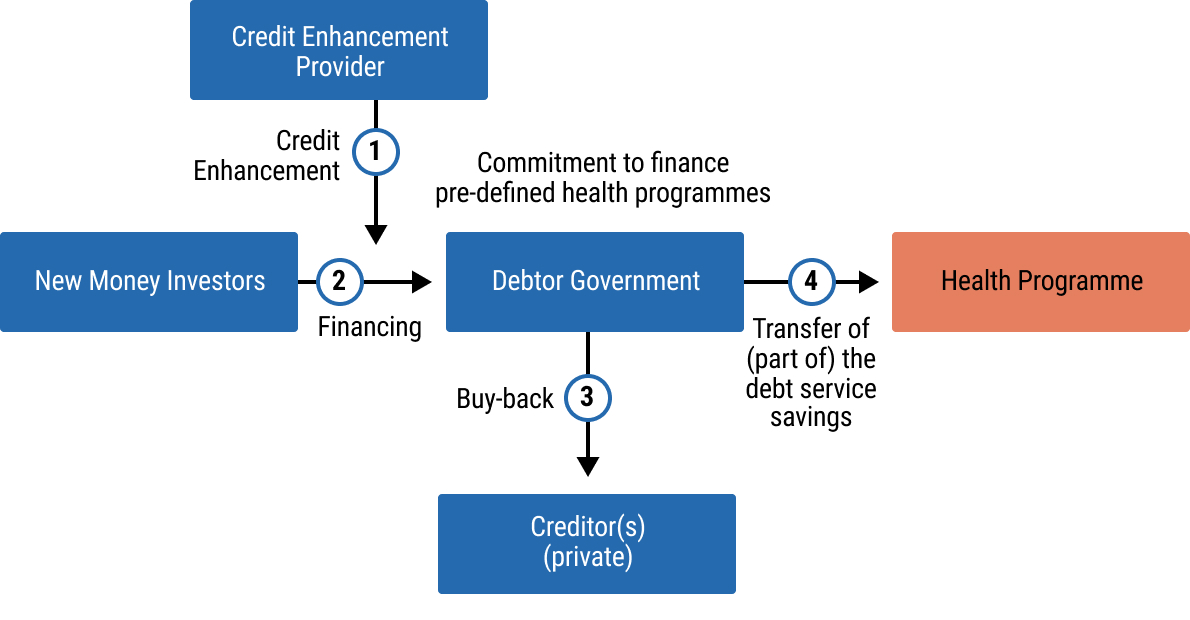 chap6_img_5
chap6_img_5
Case Study: Republic of Côte d’Ivoire, Debt-for-Development swap supported by the World Bank (2024)134chap6_p_134The transaction is the first “Debt for Development” swap supported by the World Bank following the publication of its reference framework in July 2024. It aimed to improve Côte d’Ivoire’s public debt profile and generate fiscal space for the education sector. 135chap6_p_135By refinancing expensive external commercial loans via a loan partially guaranteed by the World Bank, the transaction freed up around EUR 330 million in budget resources over the next five years, generating lifetime savings of at least EUR 60 million in net present value terms. Part of the savings will be repurposed towards an ongoing education programme supported by a World Bank Programme for Results financing instrument, which monitors the newly agreed-upon results and outcomes in the education sector, leveraging country systems already in place. The development objective of the Programme de Renforcement du Système Éducatif de Base is to improve: (i) equitable access to education and school health services at pre-school and primary level; (ii) improve learning outcomes; and (iii) strengthen performance-based management along the education service delivery chain. 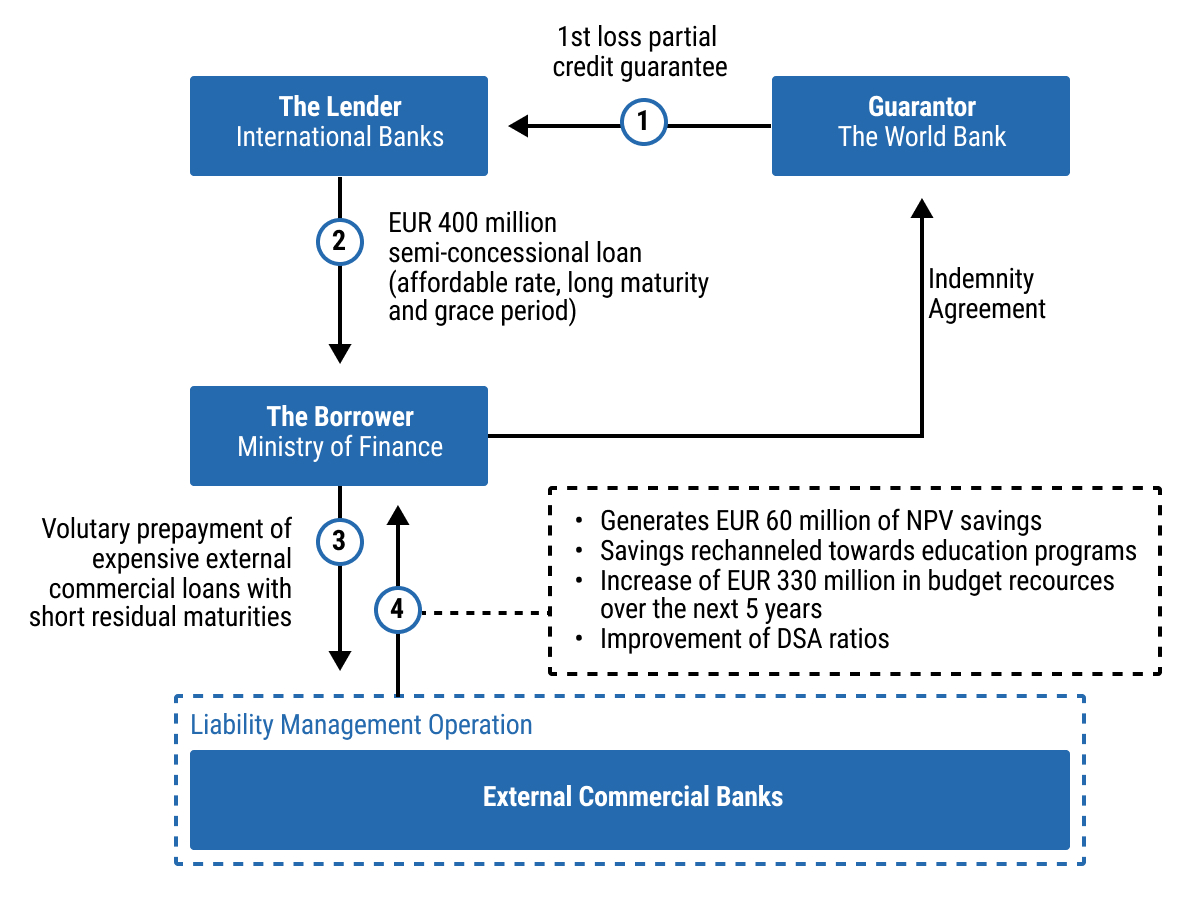 chap6_img_6 chap6_img_6 |
Enabling Conditions
136chap6_p_136Before embarking on a debt conversion, it is essential to evaluate the following criteria to assess the applicability of this financing mechanism.
- chap6_ol_6
- chap6_li_67Debt eligibility and availability. Debt conversions provide the most significant savings when the cost of existing debt is high. Hence, countries should prioritise existing debt facilities that carry high interest rates and/or shorter-term maturities. Significant savings and debt-to-GDP reductions can also be achieved if the country purchases bonds trading at substantial discounts.
- chap6_ol_7
- chap6_li_68Availability of credit enhancement. A highly-rated third party, typically an MDB or DFI, must be willing to provide a guarantee or political risk insurance (PRI) for the New Debt. Such credit support is also provided by private sector entities (e.g. insurers, impact guarantors, family offices). Such schemes will lower the interest rate on the new loan, making the debt conversion viable.
- chap6_ol_8
- chap6_li_69A clear and credible purpose. The country must have a well-defined, measurable and investment-ready national priority that is typically part of its national development strategy (e.g. funding a public health programme). This priority should feature clear SDG-related benefits for the country, which would form the basis for the commitments and targets embedded in the operation.
- chap6_ol_9
- chap6_li_70A robust governance system, characterised by transparency and accountability, is essential to manage funds effectively, meeting the requirements of investors and stakeholders. In the case of a trust fund, governance typically includes a board comprising representatives from government, private sector and civil society, supported by clear reporting requirements on fund allocation and impact.
- chap6_ol_10
- chap6_li_71Stakeholder alignment. There must be broad buy-in from local communities, civil society and relevant non-governmental organisations (NGOs). These groups are often responsible for implementing the on-the-ground projects and add crucial credibility and accountability.
- chap6_ol_11
- chap6_li_72Government’s institutional and technical capacity. To execute a debt conversion efficiently and ensure its long-term success, governments need strong political backing and adequate technical capacity. After closing, they must provide regular data and progress reports to meet performance-linked obligations.
Opportunities and Challenges
Opportunities
137chap6_p_137Managing public debt. Commercial debt-for-health swaps enable countries to utilise financial market solutions to reduce their debt stock and/or servicing costs, thereby freeing resources for health sector investment. These debt conversions are most suitable for countries with commercial debt valued below its original value and/or with expensive repayment terms, as well as those with strong financial and health partners willing to support the transaction. While not appropriate for situations of imminent default or unsustainable debt, these swaps can play a significant role in easing fiscal pressures and addressing budget constraints.
138chap6_p_138Advancing health priorities. Debt conversions can secure substantial, long-term funding for health programmes through legally binding frameworks that include monitoring and reporting requirements. This dedicated financing supports measurable health outcomes, strengthens government policy implementation and enables longer-term planning - particularly critical amid declining external funding for health. These transactions also foster improvements in data systems and reporting practices, while promoting inter-ministerial collaboration - a valuable institutional outcome in itself.
139chap6_p_139International market signalling. Such transactions signal a high level of sophistication in a country’s debt management strategy, enhancing investor confidence and broadening the investor base. They often attract attention in financial markets and media, generating positive visibility and reinforcing the country’s reputation for innovative financing.
Challenges
140chap6_p_140Process management. Executing a debt conversion requires inter-ministerial cooperation and clear ownership of the execution process by a designated ministry. A dedicated team of officials should manage the transaction, as these operations are resource-intensive and involve technical aspects that span multiple areas of responsibility. Technical assistance may be considered where capacity gaps exist. To ensure alignment, an initial workshop with all involved officials, supported by case studies and best practices, can be highly effective.
141chap6_p_141Additionally, peer-to-peer exchanges with countries that have completed similar transactions are recommended. Given the complexity and the number of parties involved, robust project management is essential. A lead entity - either within government or an external financial advisor or arranging bank - should be appointed to oversee execution, supported by detailed timelines, document checklists and step plans. Early priorities should include modelling transaction economics, including all-in costs and expenses, assessing liability management strategies for any buyback operations and projecting debt service implications to ensure all stakeholders are aligned on the financial impact.
142chap6_p_142Transaction economics. Securing credit support is a critical early step in structuring a debt swap. Indeed, credit enhancement tools - such as partial credit guarantees, insurance, collateralised schemes - will further improve the financial terms of the new instrument to be issued under the debt conversion (for further details see Chapter 8: Credit Enhancement). Early engagement increases the range of available credit enhancement solutions and helps manage complexity - particularly when multiple providers are involved, as seen in recent debt-for-nature swaps that combined political risk insurance with additional liquidity support. In such cases, intercreditor arrangements and the approach of the different credit enhancement providers to the health-related commitments should be clarified upfront, ideally through an early-stage term sheet.
143chap6_p_143Capital market volatility. For debt conversions involving the buyback of bonds listed on public markets, the bond yields or prices of those existing bonds can fluctuate significantly due to country-specific factors and global geopolitical events, potentially altering the deal economics. To mitigate this risk, confidentiality must be maintained, and external developments - such as International Monetary Fund (IMF) programme announcements, budget presentations, election cycles or ratings actions - should be factored into the timeline. Continuous monitoring of market conditions and readiness to launch when an opportune window arises are essential. This requires being fully documentation-ready and leveraging regular market updates from financial advisors, as well as arranging with banks.
144chap6_p_144Legal implications. Unlike health bonds, loans and sustainability-linked loans/sustainability-linked bonds (SLLs/SLBs), breach of health-related commitments or KPIs could lead to events of default. It is therefore essential for governments to understand the implications of such defaults, including acceleration rights (I.e. lender’s ability to declare the entire loan outstanding amount immediately due and payable following an event of default) and any consent or veto provisions required by credit enhancement providers, given the potential for cross-default provisions across other external debt obligations.
145chap6_p_145It will also be important for governments to understand the implications of any security granted as collateral and the conditions that can trigger enforcement of such security, especially if these could lead to security being enforced over funds generated by the debt swap-related savings (e.g. in relation to any endowments required to be established by credit enhancement providers such as the Development Finance Corporation (DFC)).
146chap6_p_146Data availability and monitoring system. Debt-for-health swaps require strong data systems to enable regular and transparent monitoring of progress. Depending on the design of the debt swap, this could include regular monitoring of health budget execution, tracking of programmatic indicators (such as the number of workers trained and drugs procured) or reporting of outcomes and impact (such as HIV treatment coverage or HIV incidence). The availability of reliable and consistent data is critical to building credibility in service delivery - especially as the achievement of debt-swap conditions is legally binding. Debt conversions could provide an opportunity for the MoH to invest in robust data systems and establish credibility in their data, both internally with the MoF and externally with their creditors and credit enhancement providers.
Implementation
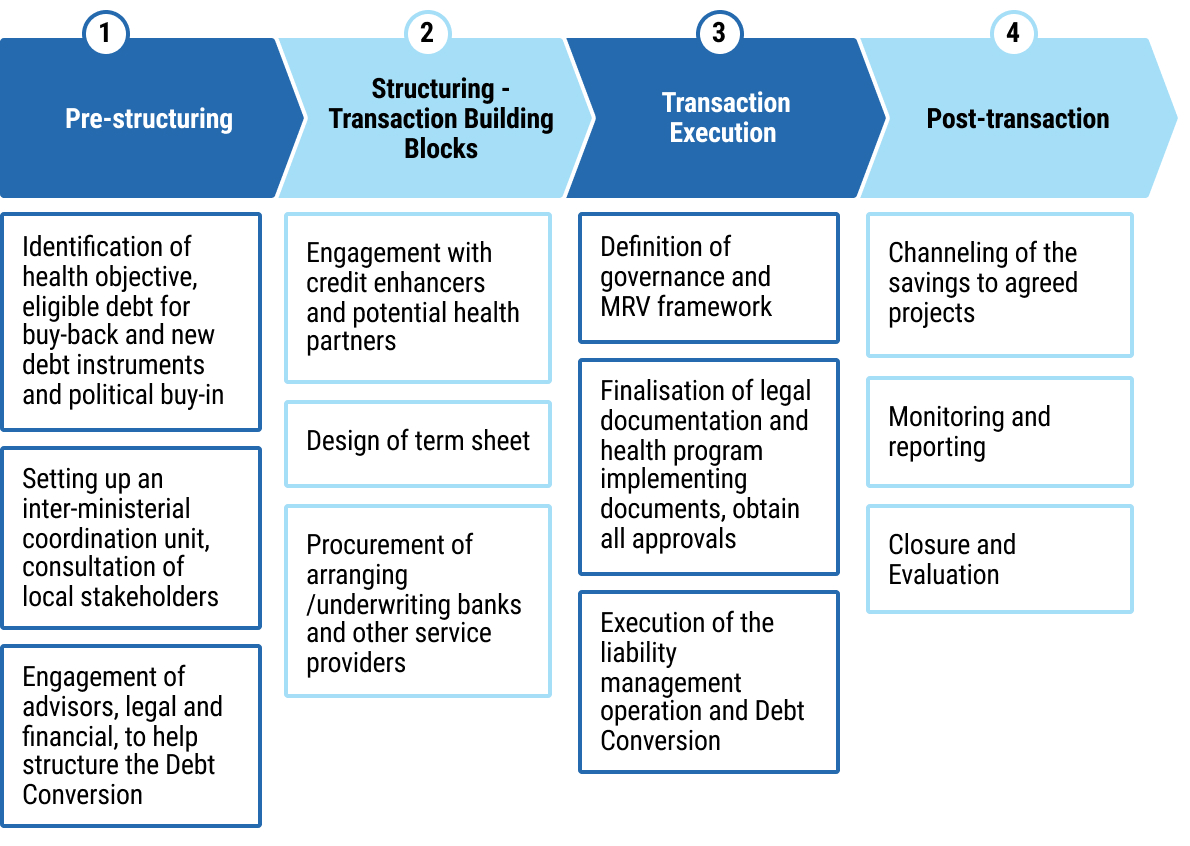 chap6_img_7
chap6_img_7Structuring of the Operation
147chap6_p_147The structuring of a health debt conversion must address two fundamental objectives:
- chap6_ul_24
- chap6_li_73Maximising the financial resources allocated to the health sector, and
- chap6_li_74Ensuring alignment with the country’s public debt sustainability framework.
148chap6_p_148To achieve these goals, three critical structuring questions must be addressed at the outset: (i) identification of eligible debt instruments to be bought back, (ii) selection of the target health programme and delivery mechanism, and (iii) design of an adequate credit enhancement mechanism. While these considerations are inherently complex and context-specific, external support from specialised third-party institutions can be mobilised to provide technical expertise, analytical input and strategic guidance throughout the process. The sections below outline these questions and potential partners.
Identification of Eligible Debt Instruments for BuyBack
149chap6_p_149A debt swap must be coherent with the country’s overall debt profile and fiscal strategy. Accordingly, a preliminary economic assessment should be conducted across the public debt facilities to identify suitable debt obligations for buyback. Priority should be given to commercial debt instruments characterised by high interest costs and short-term maturities, as well as bonds trading at significant discounts.
- chap6_ul_25
- chap6_li_75Historical precedents have focused on either bond debt (e.g. Barbados, 2022; Ecuador, 2023 and 2024; El Salvador, 2024), loans (e.g. Côte d’Ivoire, 2024) or a mix of both (e.g. Bahamas, 2024).
- chap6_li_76While the focus has typically been on external debt, certain operations (e.g. Barbados, 2024) have also targeted debt instruments denominated in local currency.
150chap6_p_150While there is no one size fits all solution, the selection of targeted debt instruments must be tailored to the specific needs and debt profile of each country, with the overarching objective of maximising available fiscal space.
151chap6_p_151It is also necessary to undertake a thorough legal review of the underlying debt contracts to assess the operational feasibility of repurchasing such debt. In the case of loan instruments, particular attention should be paid to voluntary prepayment clauses (I.e. loan-specific clauses allowing the borrower to repay the loan, in whole or in part, before its scheduled maturity date) and any associated breakage costs (I.e. the financial penalty incurred when a loan or other financial arrangement is terminated earlier than agreed), which may materially affect the economic viability of the transaction.
152chap6_p_152Legal and financial advisors can assist government authorities in performing these analyses.
Selection of the Target Health programme
153chap6_p_153The health programme to be financed through the savings generated by the debt conversion must reflect a national priority and demonstrate the potential for measurable, transformative impact over the medium to long term.
154chap6_p_154Selecting an appropriate programme is essential not only for maximising developmental outcomes but also for strengthening the narrative of the transaction. A well-chosen programme can enhance stakeholder engagement and foster broad-based support for the initiative.
155chap6_p_155Global health and development institutions can support the government in selecting existing in-country programmes. In such cases, savings can constitute a top-up to the already approved programme and funding.
156chap6_p_156
157chap6_p_157Design of the credit enhancement mechanism
158chap6_p_158Incorporating credit enhancement mechanisms into the transaction structure can enable the borrower to secure more favourable financing terms - such as lower interest rates and extended maturities - thereby amplifying fiscal savings and improving the overall risk profile of the country’s public debt portfolio.
159chap6_p_159Various credit enhancement solutions are available, including partial credit guarantees, PRI or collateral arrangements. These instruments may be combined within a layered guarantee structure to optimise risk mitigation and investor confidence.
160chap6_p_160Please see Chapter 8: Credit Enhancement for more details of the different instruments.
161chap6_p_161Credit enhancement mechanisms - particularly when structured as multi-layered schemes - may entail additional costs for the borrowing country. In this context, philanthropic organisations and grant providers can play a catalytic role by contributing grant funding to cover, either partially or fully, the premiums associated with guarantees or insurance instruments. The key element is to map out all transaction and financing-related costs early on.
162chap6_p_162MDBs, DFIs and philanthropics can support governments in providing a specific guarantee instrument. Financial advisors can further support governments in brokering different credit enhancement providers and structuring multi-layered guarantee schemes.
163chap6_p_163The structuring elements outlined above are instrumental in determining the key financial parameters of the proposed transaction, most notably the total size of the facility. This amount should reflect an optimal balance between (i) the aggregate value of the debt instruments identified for the buyback, and (ii) the financial capacity of the selected credit enhancement providers.
164chap6_p_164Given that these structuring considerations fall within the respective mandates of both the MoF and the MoH, it is essential to ensure close inter-ministerial coordination throughout the design and implementation phases. Establishing a joint taskforce or working group can facilitate this collaboration, promote coherence in decision-making and enhance the overall effectiveness of the debt swap operation.
Stakeholder Engagement
165chap6_p_165Effective stakeholder engagement is also essential for ensuring its successful implementation. This engagement must be structured across two key dimensions:
166chap6_p_166Internal coordination within the government
167chap6_p_167Sustained collaboration between the MoF and the MoH is critical throughout the entire process to ensure coherence between fiscal strategies and national health priorities. In particular, the involvement of health authorities should extend across all levels of the health system - central, regional and local - and include any related national regulators where relevant, depending on the structure of the debt conversion and the nature of the targeted health programmes.
168chap6_p_168Engagement with external stakeholders
169chap6_p_169A range of external actors may be mobilised to support the transaction at various stages:
- chap6_ul_26
- chap6_li_77Global health and development institutions. Technical assistance in identifying appropriate health programmes and expenditures, support implementation, post-implementation monitoring and reporting.
- chap6_li_78Credit enhancement providers. Including (i) Multilateral and Regional Development Banks (e.g. World Bank, African Development Bank (AfDB), Asian Infrastructure Investment Bank (AIIB), European Investment Bank (EIB)) offering partial credit guarantees, (ii) insurance providers (e.g. African Trade & Investment Development Insurance, Islamic Corporation for the Insurance of Investment and Export Credit) and (iii) private insurers (e.g. AXA, Lloyds market) offering PRI instruments. Additionally, philanthropic actors (e.g. Builders’ Vision) may also contribute by financing collateral arrangements, covering guarantee premiums or subsidising interest rate reductions linked to any sustainability-linked instruments, which may also be used in the debt conversion transaction.
- chap6_li_79Credit rating agencies (CRAs). Play an important role rating (i) any new bonds that may be issued in a debt conversion transaction as the rating informs investors and lenders on the intrinsic risk of the operation and in this regard CRAs may raise issues which impact the structuring of elements of the debt conversion, and (ii) any potential implications on the sovereign credit rating. In particular, regarding the latter, CRAs will assess whether the operation qualifies as an opportunistic exchange aligned with the country’s debt management strategy or as a distressed exchange intended to mitigate imminent liquidity pressures. Where possible, early discussions should take place with the CRAs.
170chap6_p_170The participation of well-established and internationally recognised institutions can significantly enhance the legitimacy and credibility of the operation.
Reporting
171chap6_p_171Robust reporting undertakings are a cornerstone of sustainable finance, particularly in the context of debt swap transactions. Transparent and credible monitoring of both the allocation of proceeds and the resulting impact is essential to meet the expectations of global health and development institutions, as well as international investors and lenders. These requirements are reinforced by established market standards, such as the principles of the International Capital Market Association (ICMA) and the Loan Market Association (LMA) on sustainable finance.
172chap6_p_172In the case of debt conversions, three distinct types of reporting should be implemented at various stages of the transaction lifecycle:
chap6_h4_0Verification of the generated savings
173chap6_p_173This involves monitoring the execution of the debt buyback operation to confirm the actual savings generated. The timing of this verification may vary depending on the nature of the underlying debt instrument:
- chap6_ul_27
- chap6_li_80For bond-based swaps, verification can be conducted concurrently with the issuance of the new instrument.
- chap6_li_81For loan-based swaps, verification typically occurs after the transaction, once the buyback has been completed.
chap6_h4_1Verification of savings allocation
174chap6_p_174Ensuring that the fiscal savings are effectively channelled to the designated health programmes is critical. The verification process will depend on the structure of the health programme that is targeted in the debt swap operation:
- chap6_ul_28
- chap6_li_82If the programme is managed by a recognised global health or development institution, internal mechanisms may suffice, and external verification may not be required.
- chap6_li_83However, if the savings are administered through a dedicated trust fund or a bespoke financing vehicle, an independent external verification report from a verification agent will likely be necessary to ensure transparency and accountability.
chap6_h4_2Monitoring of health outcomes and impact
175chap6_p_175The relevant party (which could be the MoH and MoF, and any administering third party) must commit to reporting on the health outcomes and broader developmental impact of the financed programme. This includes tracking agreed KPIs, evaluating progress against predefined targets and assessing long-term benefits to the population, depending on the beneficiaries targeted by the programme. Some credit enhancement providers may require additional independent verification.
176chap6_p_176The capacity to deliver on these reporting requirements will vary across countries. In contexts where institutional capabilities are sufficiently developed, reporting may be conducted internally through coordinated efforts between the MoF and MoH. In other cases, technical assistance from international or regional partners may be required to support data collection, analysis and reporting.
177chap6_p_177Establishing a clear and credible monitoring framework not only enhances transparency but also strengthens investor confidence, reinforces the legitimacy of the transaction, and contributes to the broader objectives of sustainable development.
Case Study: Republic of Ecuador, Debt-for-Nature Swap (2023)178chap6_p_178In May 2023, Ecuador’s government executed a debt conversion to protect the Galápagos Islands. This innovative transaction enabled the country to exchange USD 1.63 billion of its existing high-interest commercial bonds for a new, significantly smaller USD 656 million loan, reducing the nation’s debt by nearly USD 1 billion. It is projected to save Ecuador over USD 1.1 billion in debt service payments over the term of the transaction. 179chap6_p_179The new loan was credit-enhanced with political risk insurance from the U.S. International DFC and a USD 85 million guarantee from the Inter-American Development Bank (IDB). This combination significantly lowered the borrowing cost for Ecuador, making the entire conservation funding scheme financially viable. 180chap6_p_180The transaction is projected to generate USD 450 million for marine conservation, which will be managed and disbursed over the next 18.5 years by a newly created nonprofit entity, the Galápagos Life Fund (GLF). The fund’s governance system is a public-private partnership, ensuring accountability through an 11-member board of directors. This board comprises five members from the Ecuadorian government and six non-governmental members, representing various stakeholders. This structure governs how the funds are spent on key priorities, which are tied to new conservation commitments made by Ecuador. These commitments broadly aim to strengthen the management, monitoring and enforcement of its marine protected areas and improve the overall sustainability of its fisheries. The GLF will also support scientific research and build an endowment to provide funding in perpetuity. 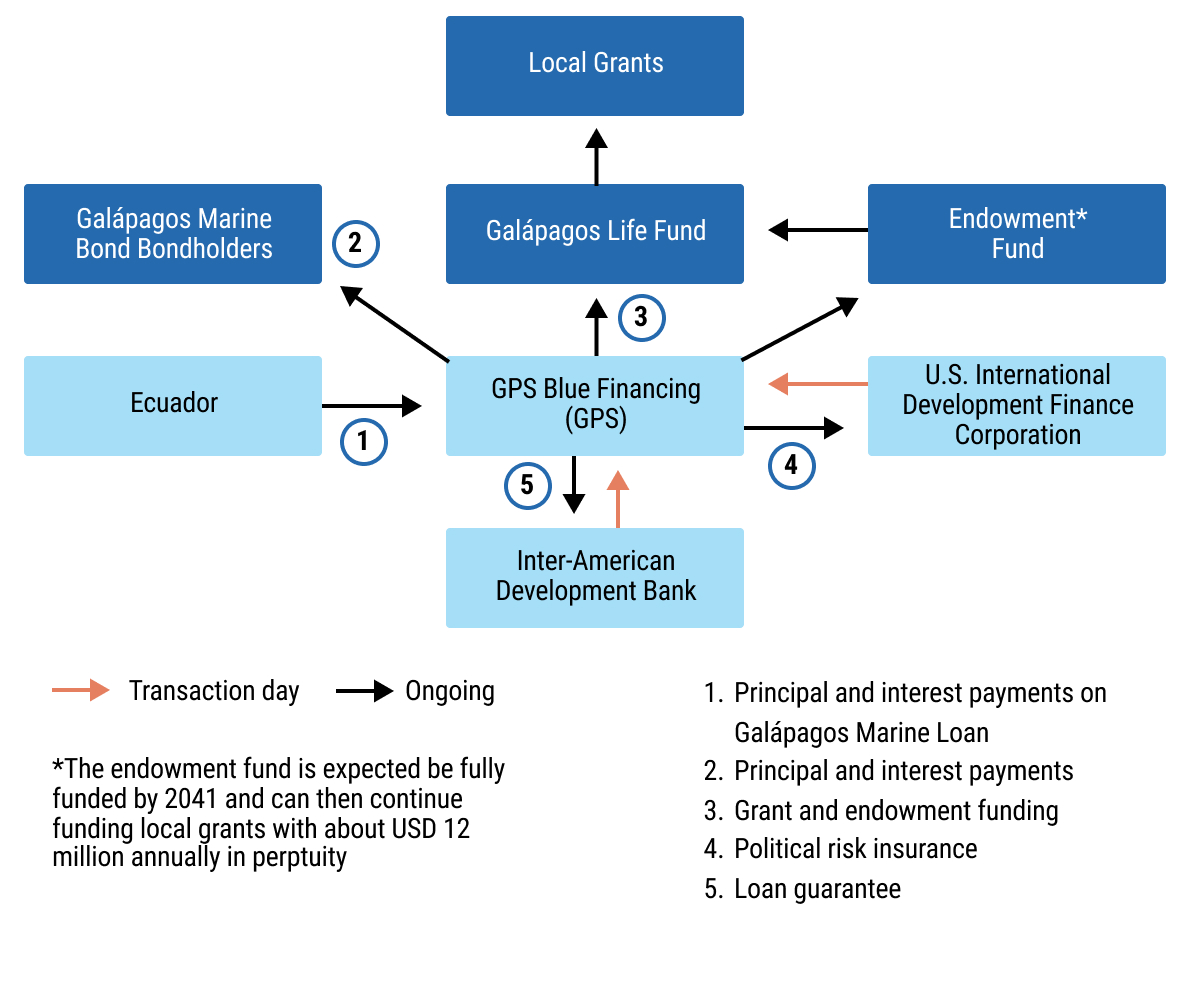 chap6_img_8 chap6_img_8 |
Key Legal Considerations
181chap6_p_181This section will provide an overview of the principal legal and documentation issues that typically arise in the negotiation and implementation of debt conversion transactions. It is intended to guide government officials and other potential stakeholders and transaction participants through the key instruments, contractual provisions and procedural steps involved in structuring a bilateral debt swap or debt conversion.
182chap6_p_182It begins by outlining the contractual framework for bilateral debt swaps, describing some of the main documents and key provisions that should be considered when negotiating these transactions. The second part discusses legal considerations related to debt conversions, including relevant legal documentation, credit enhancement considerations, the contractual treatment of health-related commitments and KPIs, the establishment of trust or project implementation funds, the inclusion of back-to-back funding arrangements and security structures. The discussion also outlines additional legal processes and operational considerations that are critical to execution.
Bilateral Debt Swaps
183chap6_p_183From a documentation perspective, bilateral debt swap agreements are simpler than debt conversions (described below). A bilateral debt swap is usually implemented through formal international contracts, usually comprising three tiers:
- chap6_ul_29
- chap6_li_84Intergovernmental framework agreement. This treaty-level instrument establishes the principle of the swap and is typically signed between the creditor and the debtor country. The agreement defines the total amount of debt to be cancelled or reduced and the broad purpose (e.g. for health system strengthening).
- chap6_li_85The debt swap agreement. This agreement outlines the financial and legal details of the arrangement, including the nominal amount, exchange rate, payment schedule, eligible sectors, project approval process and default provisions. The payment schedule may deviate from the initial debt repayment schedule to reflect the absorptive capacity of the programme or, if the debtor has negotiated a grace period, to ensure funds are transferred to the relevant fund, third-party entity or health project or programme. The agreement also defines how the debtor country will make counterpart payments to the fund, the implementing entity or the health project.
- chap6_li_86The implementation agreement. This agreement is usually signed between the debtor country and the implementing entity (e.g. the Global Fund). The agreement governs disbursement, fiduciary controls and monitoring.
184chap6_p_184It is important to note, however, that in a bilateral debt swap transaction, there is no standardised approach to legal documentation. In some cases, key provisions will be included in a single comprehensive debt swap agreement, while in others, various conditions and terms may be contained in separate agreements (e.g. a separate implementation agreement or trust agreement).
185chap6_p_185Two additional legal frameworks might be necessary on the creditor side:
- chap6_ul_30
- chap6_li_87Some creditors may have a nationally approved framework to support debt swaps, or they may require one that needs to be approved by their Parliament. For example, Germany’s Federal Budget Code empowers ministries to defer, reduce or write off federal claims - the core legal tool enabling debt cancellations/conversions. The Budget Act sets binding amounts annually for debt swaps.
- chap6_li_88Since the late 1980s, the Paris Club has included a debt swap clause in its agreements under specific conditions. That clause allows Paris Club creditors to convert part of their eligible claims (typically concessional loans) into a debt swap under agreed parameters. The quantitative limit is a 10-20% cap of the total restructured amount, and creditors are requested to inform other Paris Club members of any planned debt swap.
186chap6_p_186Provisions to be mindful of:
- chap6_ul_31
- chap6_li_89Debt reduction or cancellation clause. This clause specifies the scope and structure of the fiscal relief being provided in exchange for the debtor’s commitment to fund specific programmes or projects. Debtors should confirm whether relief takes the form of partial or full debt cancellation, debt reprofiling or rescheduling. In addition, to the extent that any partial write-off or cancellation has been negotiated, the debtor should suggest that this occur upfront rather than being conditional upon programme completion, so that the country obtains immediate fiscal relief. Finally, it is crucial to clarify in the documentation how and when debt obligations are extinguished - whether progressively as funds are transferred, or once the full amount is committed - and that once debt is deemed extinguished, it cannot be reinstated or clawed back by the creditor.
- chap6_li_90Transfer mechanics and schedule. This language in the debt swap agreement defines how, when and in what currency the debtor transfers freed-up resources to any designated fund, escrow account or programme administrator. When negotiating this clause, the debtor should carefully consider the duration and frequency of the transfer obligation, taking into consideration factors such as budget cycles, transaction costs, administrative simplicity and project absorption considerations. In some instances, depending on the debtor’s fiscal position, the debtor may also seek to negotiate a grace period before transfers begin to avoid budgetary strain.
- chap6_li_91Currency of transfer. Debtors typically prefer local currency transfers to align with local expenditures. However, if currency conversion is required, it is vital to ensure a fair and transparent exchange rate reference (e.g. central bank rate).
- chap6_li_92Monitoring and evaluation clause. This clause, to the extent it is included in the debt swap agreement, establishes oversight, reporting and audit mechanisms to ensure that resources are appropriately used for the agreed-upon purposes. Of note, this may also be included in a separate legal document, such as an implementation agreement. When reviewing this clause, debtors should clarify the format, frequency and responsible party for any reporting. It is also essential to avoid overly burdensome monitoring requirements that create excessive administrative costs or delays.
- chap6_li_93Transfer default and remedies clause. This clause defines the consequences of the debtor’s failure to fulfil its transfer obligations under the agreement and the remedies available to the creditor. Creditor remedies may include (i) reinstatement of the original debt (I.e. reverting to the original loan terms) and (ii) acceleration of payments under the original debt (I.e. requiring all remaining payment obligations to become immediately due). Debtors should negotiate a reasonable cure period (e.g. 2-6 months) during which the government can cure any default before the creditor can exercise its remedy rights.
Debt Conversions
187chap6_p_187Documenting a debt conversion requires a broader set of agreements than a standard bond issuance or loan transaction. The Attorney General’s Office (or equivalent) and the heads of relevant ministries’ legal departments should be aware early on of the transaction, as additional legal approvals may be required. The legal review process can also take longer due to the more structured and bespoke elements involved, which are not typical of other transactions that MoFs are accustomed to.
188chap6_p_188Negotiations often involve multiple ministries and agencies; therefore, forming a cross-government working group or task force can be beneficial. Clearly defining each ministry’s role, e.g. the MoF for liability management and funding aspects, and the MoH for health-related commitments, will help coordinate documentation, execution and ongoing monitoring. Holding regular check-ins will also facilitate this coordination.
189chap6_p_189Required documentation generally falls into the following categories:
- chap6_ul_32
- chap6_li_94Documents supporting the participation of initial stakeholders (e.g. mandate letters for lenders and arrangers, engagement letters for legal and financial advisors, appointment letters for third-party technical assistance, application for credit enhancement mechanisms)
- chap6_li_95Liability management documents (e.g. tender offer memorandum)
- chap6_li_96Debt conversion documents
- chap6_li_97Credit enhancement agreements (e.g. guarantee agreements, insurance policies)
- chap6_li_98Health-related policy and funding commitments for using the fiscal savings generated by the debt conversion
- chap6_li_99Documents establishing any trust fund or project implementation fund
- chap6_li_100Agreements for back-to-back funding, if applicable
- chap6_li_101Security and intercreditor documentation, in some cases
190chap6_p_190These are each described in more detail below.
Documentation Supporting the Participation of the Initial Participants in the Proposed Transaction
191chap6_p_191Once the sovereign has determined that it wishes to undertake a debt conversion, several third parties will need to be brought on board, and each of them will need to be mandated through a separate bilateral engagement letter with the government (usually through the MoF). This will include, inter alia:
- chap6_ul_33
- chap6_li_102Legal advisors and potentially financial advisors, who will advise on the contemplated transaction.
- chap6_li_103International and/or domestic banks, which could act as arrangers and/or underwriters of the new bond/loan at the heart of the debt conversion, as well as dealer managers in respect of any tender of the sovereign’s existing bonds (in case the debt conversion targets outstanding bonds).
- chap6_li_104Credit enhancement providers (e.g. MDBs, DFIs) typically support operations and usually require formal application requests from governments, as well as thorough due diligence processes. As such, a common understanding of these requirements, as well as any associated fees and expenses (including guarantee/insurance premia), should be sought early on. It is to be noted that these credit enhancement providers will require separate legal advice (often both international and national).
- chap6_li_105Global health institutions or NGOs can provide technical assistance on the health aspects of the operation and the health-related applications of the fiscal savings generated by the debt conversion, as well as monitoring and reporting components.
- chap6_li_106Rating agencies are typically involved at two levels: (i) rating the new debt instrument; and (ii) assessing any potential implications of the debt buyback on the sovereign rating.
- chap6_li_107Other third parties (e.g. trustee, facility agent, tender agent to manage and administer the tender offer and other parties’ legal advisors), whose roles will depend on the target operation’s structure and can be mapped out by the banks mandated to arrange the operation. Typically, banks will obtain quotes from two or three providers of such services to ensure competitive pricing and optimisation of transaction costs for the government.
192chap6_p_192Procurement/Request For Proposals (RfPs)
193chap6_p_193Thought will need to be given to any country-specific procurement processes to mandate the required parties or other ways of doing so, which will comply with national requirements - such requirements may lead to the need for an RfP to be drafted to invite financial advisors, legal advisers and banks to submit proposals to the MoF. These can be very useful, as would interviewing parties submitting proposals. The scope of each such mandate, as well as timing and fee coverage, will need to be clearly established (typically in a mandate or engagement letter).
194chap6_p_194At this initial step, and given the number of participants, it will be critical to ensure alignment across all parties on (i) the technical and commercial parameters of the deal, and (ii) the overall execution timeline - especially as the disbursement date should be in line with the overall MoF’s funding plan for the year.
195chap6_p_195Other documents
196chap6_p_196As such, beyond the bilateral mandate and engagement letters, four other documents can be elaborated and circulated to all relevant parties:
- chap6_ul_34
- chap6_li_108A financial model is used to map out the overall costs of the transaction and debt servicing costs. There should be a regular review of the model as the transaction moves from concept to execution. This model can be elaborated and maintained by the MoF team and its financial advisor.
- chap6_li_109A Term Sheet with the main commercial and legal parameters of the proposed transaction. This can ensure that, before moving to the full documentation stage, all the parties agree on the main parameters of the debt conversion.
- chap6_li_110A detailed execution timeline mapping out the different workstreams (e.g. alignment on commercial terms, negotiation of all legal documents, selection of all third parties, approval of the project by the credit-support providers’ boards, government approvals, ratings).
- chap6_li_111A document list with allocated responsibilities, indicating who has primary responsibility for drafting each document, the parties involved, who will review the document, and its position in any timeline.
197chap6_p_197Partners
198chap6_p_198In large debt conversion transactions involving multiple parties and legal advisors, having a strong coordinating partner can make a significant difference to the success of transaction execution, and it should be clear from the outset who will assume this role. In past transactions, this has ranged from a presidential advisor to a minister, the external financial advisor to the MoF or even an arranging bank. If a party outside of government, there should be clear lines of access to senior government officials and staff.
Confidentiality
199chap6_p_199Whilst the country is working on a debt conversion, it is often preferable that this should remain confidential. Where the subject of the debt conversion is publicly traded bonds in the capital markets, this is especially important, as the bond price may rally upon such information being known, and the fiscal savings the country seeks to obtain may diminish. The need to maintain confidentiality also applies to any credit enhancement providers who may inadvertently disclose a proposed transaction through the process of obtaining board approval. For example, early discussions should address these guidelines and any related measures put in place with all parties to the transaction and their respective employees/officials.
Liability Management Documentation
200chap6_p_200At the heart of many transactions is the buying back of sovereign bonds. The greater the discount at which such bonds are trading, the greater the fiscal savings that could be generated from the debt conversion. The buyback component of the transaction is similar to any simple liability management transaction that a country would undertake as part of its day-to-day debt management strategy, based on a cash tender offer.
201chap6_p_201Documentation will involve agreeing on a tender offer (I.e. an offer by the sovereign issuer to repurchase outstanding debt securities from existing holders) memorandum, a letter appointing a tender agent and related internal approvals. Where the tender is to be executed by way of a cash tender, it would not usually require country disclosure on the sovereign. Thought will primarily need to be given to selecting the target bonds based on maturity, trading price, and the bunching of maturities, among other factors. Additionally, it is essential to consider whether any bonds include call options, which could also support the liability management strategy. In many cases, the tender offer would be fronted by the sovereign (indeed, this may be a legal and/or contractual requirement in some instances). Still, there have been some transactions fronted by third parties (with the tacit approval of the sovereign).
202chap6_p_202There are several key elements to consider in this regard, including national requirements, any constraints within the terms of the existing bonds (e.g. if combined with the use of a bond call option upon reaching certain thresholds of bonds tendered), and the preferences of the credit support provider. Some credit enhancement providers prefer that funds be used directly to pay the cash tender without first flowing through the sovereign. Arrangements can be put in place for the funds raised to flow to tendering bondholders. However, parties should agree on a funds flow and related letters of instructions to third parties to effect such a funds flow as part of the liability management discussions.
Debt Conversion Documentation Including Credit Enhancement (if any)
203chap6_p_203The existing bonds that are being bought and cancelled will be replaced by a loan or bond, often with credit enhancement and lower debt servicing costs. Whether the replacement instrument is a bond or a loan will be determined by sovereign preferences, credit support provider preferences and lender/investor preferences. In some instances, a country may not have the approvals to issue/enter into a particular instrument and will prefer the other. Credit enhancement providers may only be authorised to provide credit support in relation to a bond or a loan. The arranging bank may wish to remain the lender of record and prefer a loan. Early in the process, these preferences should be discussed and an understanding reached regarding the funding instrument. The term sheet should reflect the positions reached.
Loan option
204chap6_p_204Where the debt replacement instrument is a loan, the country will be required to enter into a facility (or loan or credit) agreement through its MoF or a usual contracting party. A facility agent will also be required to administer the loan. The lender(s) may be a bank(s) or a special purpose vehicle (SPV) established to act as a conduit in the transaction, if a back-to-back financing arrangement is being put in place to raise funding from the capital markets. The loan will be similar to other facilities the country may have entered into but will also include some additional features: provisions required by the credit enhancement providers; additional mandatory prepayment events or events of default related to loss of the credit support; additional representation, covenants and events of default and transaction specific acceleration rights triggering early repayment; provisions relating to subrogation rights and transfer/assignment rights related to the credit support and any back to back funding strategy.
205chap6_p_205Care will be needed to review any counter-guarantees or counter-indemnities required by credit enhancement providers carefully and to understand the consequences of default on the sovereign’s broader access to the credit support provider’s offerings (especially if a multilateral development bank on which the sovereign is highly reliant). For further information, see Chapter 8: Credit Enhancement.
206chap6_p_206Thought will also need to be given to the hierarchy of credit support if more than one, and any sharing clauses and subrogation rights that the parties will require. Whilst the country may not have access to the full suite of guarantee documents that the credit support provider may require in the transaction, it should seek to understand the implications of such documents, including consent/subrogation/Personal Care Services rights, especially in a default scenario.
207chap6_p_207The facility agreement will also typically include an undertaking by the MoF to make available the agreed-upon portion of the savings generated by the transaction to the party that is due to receive such payments (be it a government agency, trust fund or project implementer). A decision will need to be made in advance whether such an undertaking requires all the savings to be granted in one payment at the outset of the transaction or to be gradually released over a specified timeframe. In the health space, this will require special consideration in view of the potentially increased benefits of early investment in the well-being of any targeted group.
208chap6_p_208In either case, if such payments are not made, this would result in an event of default under the loan. The facility agreement will also include specific mechanisms whereby, if the agreed-upon health KPIs or policy health commitments are not met, the government may have an obligation to make additional payments.
209chap6_p_209The health KPIs and commitments, along with their related remedies, are to be carefully negotiated separately, as described below. Unlike thematic bonds, debt conversions have hitherto been structured (following appropriate grace periods) to be capable of resulting in a default (with broader cross-default implications), so additional care must be exercised in understanding the links between the facility agreement and the agreements containing the health-related commitments.
Bond Option
210chap6_p_210Where a country cannot enter into a loan, it may decide to issue a bond, which can be held by a single entity (e.g. an SPV). In such cases, the bond terms and conditions will not be the same as other bonds issued by the sovereign, but will, as per the loan description above, also include bespoke elements. Thought will need to be given as to the implications of U.S. securities laws on the structure, applicable exemptions from U.S. registration requirements and the role of the bank(s) or an SPV as initial purchasers. Banks will be very focused on potential underwriter liability and will need to map out an approach on whether country disclosure is necessary or not. Providing such disclosure can be quite onerous for some countries; therefore, addressing this in conversation with the arranging bank(s) early in the process is essential.
211chap6_p_211Where a debt conversion transaction involves a credit support provider which does not favour funding flowing through the sovereign, a separate exchange and settlement agreement may be entered into specifying that the lending obligation under the loan by the lender is discharged by the latter’s settling of the tender offer in exchange for an undertaking by the sovereign to instruct the cancellation of the bonds tendered in the cash tender.
Documentation Related to Health Policy Commitments and KPIs
212chap6_p_212From a documentation and structuring perspective, these can differ transaction to transaction. It may be that the country has partnered with an underlying international organisation working in the health sector, which has its own objectives in participating in a debt-for-health swap with the government and the types of country commitments, spending of the savings generated by the transaction and implementing strategy for doing so will be framed by the ongoing partnership (the first scenario).
213chap6_p_213The country and such organisations have specific bilateral multi-year plans, and the funding freed up by the transaction can support programmes that would otherwise not be funded. Alternatively, the credit support provider is particularly focused on specific outcomes to participate in the transaction, and it will have contractual requirements that need to be embedded in separate agreements (the second scenario).
214chap6_p_214The various approaches can significantly impact the documentation. In relation to the first scenario, it is essential to note that investors will expect any transaction to be accretive to existing spending arrangements (and not just a replacement). However, good use could still be made of existing plans.
215chap6_p_215Typically it will be necessary, however, to enter into an additional commitments agreement setting out government specific health policy and other commitments and/or KPIs, breach of which will lead in the first instance to an obligation to make additional payments and in due course termination of the agreement (in turn potentially leading to an event of default under the sovereign loan/bond).
216chap6_p_216In the second scenario, the credit support provider may have additional requirements, including the participation of a third-party non-profit or trust fund in the structure, which will require additional documentation (see below).
217chap6_p_217On debt conversions undertaken in the last few years, the inclusion of such trust funds in the structure has resulted in the savings generated by the transaction being paid by the MoF under the primary loan/bond to the lender/purchaser thereof and this party agreeing under a separate agreement to pay the funds to the third-party trust fund with certain suspension in the funding being envisaged in case of non-compliance by the fund with KPIs agreed to by it.
218chap6_p_218The MoH should allocate considerable time to negotiating relevant health-related policy commitments and KPIs, including appropriate grace periods and monitoring and reporting mechanisms, as breaches could result in financial penalties and ultimately lead to default. Credit enhancement providers and investors are typically willing to agree to implementation delays and catch-up periods if the terms are appropriately structured.
219chap6_p_219Regular reporting will also be expected, with third-party verification agents being required in certain transactions (accompanied by related documentation that reflects the scope of work, frequency of verification, coverage of fees and other relevant details). To the extent that the country already does regular reporting that can be repurposed, that would be beneficial, especially if such reporting already involves external third parties.
Case Study: Identifying KPIs and Health Commitments for a Debt Conversion220chap6_p_220As outlined in this chapter, a debt swap must embed government health-related policies and other commitments, funding and health-related KPI targets within a contractually binding framework. This makes the selection of the right obligations a critical success factor for debt conversion. Failure to meet these commitments will result in financial penalties and ultimately lead to default under the sovereign loan or bond. 221chap6_p_221Creditors and credit enhancers are typically looking for commitments that prove additionality to their funding and which are accretive to existing government expenditure in the health sector. For example, certain credit enhancement providers may be interested in seeing improvements in communicable diseases, specifically, while others may be interested in health systems strengthening more broadly. 222chap6_p_222Generally, two types of commitments can be included in a debt conversion: government policy or planning commitments and KPIs. 223chap6_p_2231. Policy or Planning Commitments:
224chap6_p_2242. Key Performance Indicators (KPIs)
225chap6_p_225There is flexibility to define the commitments based on the country’s own needs and priorities. They should align with national strategic plans and health priorities. They should also be verifiable by a third party. It is essential to consider how the MoH or the MoF data systems enable this external verification, and where needed, are strengthened to provide accurate and timely data on the KPIs for reporting purposes. 226chap6_p_226The expectation is that the government itself will provide the policy and other related commitments through the MoH, but that the KPI-related undertakings will be provided by the party assigned to receive the fiscal savings under the debt conversion. |
Establishment of a Third-Party/ Non-Profit Trust Fund
227chap6_p_227As referred to in the second scenario above, where such entities are required, careful consideration will need to be given to several issues: is the entity to be for sole use or could it be a conduit for future grant funding etc.; who will be on its board (typically the entity would not be government controlled but would have some ministerial representation on the board); what will its corporate governance be; will it have a physical office and staff; how will its funding from the savings generated by the transaction be applied (agreed upfront or some discretion over time and related governance); frameworks for investment of any unutilised financing, auditing, risk and compliance, appropriate environmental and social standards policies.
228chap6_p_228In transactions where such an entity is required, establishing the trust fund should become its own workstream, and consideration should be given to the timing of establishment, preparatory work, and adequate discussions with government officials, among other factors. A key evaluation will also determine whether the trust fund will directly implement part of the project itself or provide funding to third parties, in which case it will also need to consider the monitoring and accountability of such third parties. Another key question will be whether the trust fund needs to be established in the country (as per local regulations, for instance) or offshore (as per the credit support provider’s preference).
Back-to-back Funding Structures
229chap6_p_229Unless the arranging bank(s) can lend and keep a loan on the balance sheet on day one, a back-to-back funding structure may likely be required. In such instances, an SPV may be suggested as the lender of record under the primary loan or bond, to then become the issuer/borrower under the back-to-back bond or loan. The use of SPVs may also be necessary as a result of credit enhancement providers’ requirements related to their coverage.
Security Documents and Intercreditor Arrangements
230chap6_p_230More complex structures may require agreement on security arrangements. This is particularly likely to arise in a transaction which has a back-to-back funding arrangement, as investors will want to have recourse via any SPV to the credit support and any cash available. If the transaction involves more than one credit support provider, this may also give rise to the need for intercreditor arrangements, which must be documented.
231chap6_p_231Similarly, some credit enhancement providers may require some security to be granted on savings generated by the transaction (famously, where such parties have required the establishment of a longer-term endowment to be partly funded by the savings generated over time). Discussions on security can often lead to requirements for accounts to be held offshore, and the sovereign should be aware of such features as early as possible.
Approvals
232chap6_p_232Several government approvals and local legal opinions will be required to support any debt conversion. Early consideration should therefore be given to this, as such elements will be required as conditions precedent to any transaction closing. Thought should be given as to what approvals/opinions will be required from the Attorney General/Minister of Justice, and early involvement of such parties to describe the structure is always beneficial and can avoid last-minute delays.
233chap6_p_233Similarly, if any parliamentary approval is needed, consideration should be given to the required documentation and timing implications for the overall transaction execution. The country should also seek information regarding the approvals required by the other parties to the transaction and their own documentation requirements for such approvals, as this can also significantly impact overall timings. In each case, the concerns raised under confidentiality should be taken into account on an ongoing basis.
Know Your Customer (KYC)
234chap6_p_234Know your customer (KYC) requirements can also be a factor that can delay transaction execution. These requirements generally involve collecting and verifying information to confirm the identity, nature and risk profile of a counterparty. Early in the process, a party should map out the KYC requirements and ensure that the relevant parties begin to provide documentation to satisfy these requirements.
Establishment of Required Bank Accounts
235chap6_p_235The transaction may also require the opening of multiple bank accounts, both onshore and offshore. These should be mapped out early on, and the bank account opening documentation becomes a separate legal documentation workstream to avoid unnecessary delays.
Funds Flow
236chap6_p_236In view of the multiple parties involved and various layers to any debt conversion, it is advisable to draft and agree on a funds flow to capture the various steps required to enter into all the relevant documents, satisfy conditions precedent and ensure the effectiveness of any credit support before new money flows and the required cash flows and supporting instructions.
Debt Pause Clauses
237chap6_p_237The MoF may request the arranging bank(s) to include a debt pause clause or a pandemic debt pause clause in the loan or bond replacing its existing debt. This would enable the country to defer payments on a loan or bond under certain circumstances. It would be beneficial to discuss with the arranging bank(s) early the inclusion of such a debt deferral mechanism, including in the request for proposals (RfP) for bank proposals, if one is issued.
238chap6_p_238Please see Chapter 5: Sustainable Finance Instruments (Key Legal Considerations) for a detailed description of pandemic and epidemic-related pause clauses, and for a template pandemic clause.
Summary of Transaction Implementation Steps
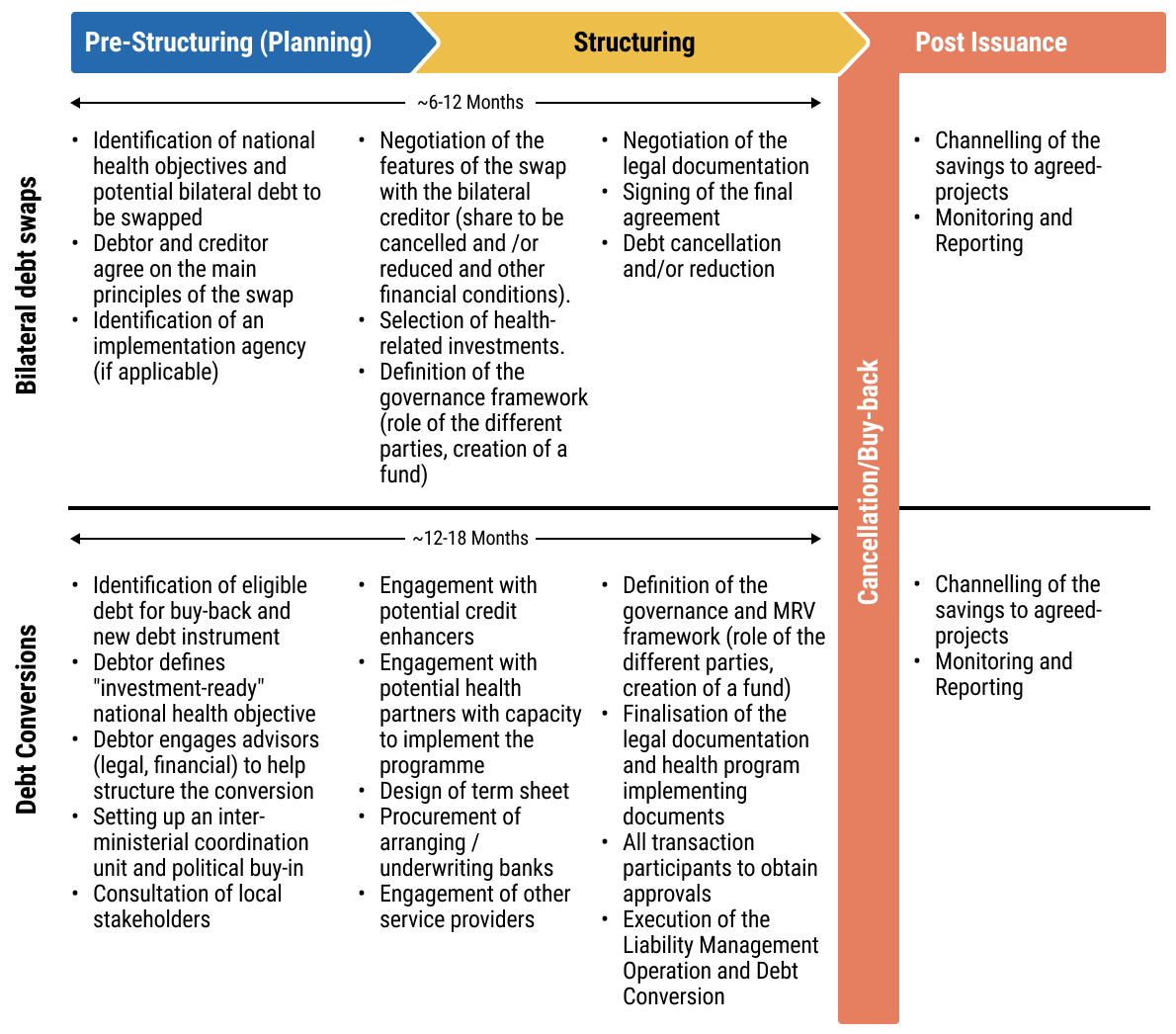 chap6_img_9
chap6_img_9239chap6_p_239
240chap6_p_2401
241chap6_p_241Decision and Internal Preparation
- chap6_ul_37
- chap6_li_118Decide to pursue a debt conversion (Cabinet / MoF approval).
- chap6_li_119Map eligible debt (identify commercial debt suitable for buyback or exchange).
- chap6_li_120Confirm policy objective (e.g. health, climate or development).
- chap6_li_121Ensure internal coordination between MoF, MoH (or relevant line ministry), Attorney General (or equivalent) and Central Bank.
- chap6_li_122Maintain strict confidentiality, especially if bonds are publicly traded.
242chap6_p_2422
243chap6_p_243Mandate and Procurement of Key Participants
- chap6_ul_38
- chap6_li_123Appoint and contract:
- chap6_li_124Legal advisors (international and domestic).
- chap6_li_125Financial advisors.
- chap6_li_126Arranging/underwriting banks (for new bond or loan issuance).
- chap6_li_127Credit enhancement providers (MDBs, DFIs) - begin formal application and due diligence process.
- chap6_li_128Rating agencies (for rating the new instrument and assessing the impact on the sovereign rating).
- chap6_li_129Other service providers: trustee, facility agent, tender agent, verification agents, etc.
- chap6_ul_39
- chap6_ul_40
- chap6_li_130Clarify procurement process - RfPs, interviews, evaluation and selection in line with national rules.
- chap6_li_131Sign engagement/mandate letters, defining scope, fees and timelines.
244chap6_p_2443
245chap6_p_245Initial Structuring and Coordination
- chap6_ul_41
- chap6_li_132Designate a coordinating partner (e.g. minister, presidential advisor, financial advisor or lead bank).
- chap6_li_133Prepare and circulate key core documents:
- chap6_li_134Financial model - mapping costs, debt service and savings.
- chap6_li_135Term Sheet - outlining main commercial and legal parameters.
- chap6_li_136Execution timeline - sequencing approvals, documentation, rating & credit-support milestones.
- chap6_li_137Document responsibility matrix - identifying drafters, reviewers and deadlines.
- chap6_ul_42
- chap6_ul_43
- chap6_li_138Align all parties on parameters, deliverables and funding schedule.
246chap6_p_246
247chap6_p_2474
248chap6_p_248Liability Management and Buyback Execution
- chap6_ul_44
- chap6_li_139Identify target bonds or loans for buyback (based on maturity, pricing, liquidity).
- chap6_li_140Prepare liability-management documentation:
- chap6_li_141Tender offer memorandum.
- chap6_li_142Appointment of tender agent and trustee.
- chap6_li_143Internal MoF approvals and instructions.
- chap6_ul_45
- chap6_ul_46
- chap6_li_144Agree on funds flow arrangements - especially if credit enhancement providers prefer funds not to pass through sovereign accounts.
249chap6_p_2495
250chap6_p_250Structuring the Replacement Instrument
251chap6_p_251Option A - Loan Structure:
- chap6_ul_47
- chap6_li_145Draft and negotiate facility agreement, incorporating:
- chap6_li_146Credit enhancement-related clauses and subrogation rights.
- chap6_li_147Representations, covenants, events of default.
- chap6_li_148Undertakings on allocation of savings (e.g. to health trust fund or programme).
- chap6_li_149Potential debt pause or pandemic clause.
- chap6_ul_48
- chap6_ul_49
- chap6_li_150Coordinate back-to-back funding structure if SPV or private placement is involved.
252chap6_p_252Option B - Bond Structure:
- chap6_ul_50
- chap6_li_151Draft bespoke bond terms and conditions (reflecting credit enhancement-related provisions).
- chap6_li_152Ensure compliance with securities laws (ensure compliance with U.S. securities laws).
- chap6_li_153Determine whether the issuing structure requires an SPV to act as intermediary.
253chap6_p_2536
254chap6_p_254Credit Enhancement
- chap6_ul_51
- chap6_li_154Finalise guarantee or insurance arrangements with MDB/DFI.
- chap6_li_155Review counter-guarantees and subrogation provisions carefully.
- chap6_li_156Clarify ranking and interaction of multiple credit supports if applicable.
255chap6_p_255
256chap6_p_2567
257chap6_p_257Third-Party Structures
- chap6_ul_52
- chap6_li_157If required, establish a trust fund or third-party vehicle to manage savings, with defined:
- chap6_li_158Governance and board composition.
- chap6_li_159Spending rules and audit requirements.
- chap6_li_160Location (onshore vs. offshore) and regulatory approvals.
- chap6_ul_53
258chap6_p_2588
259chap6_p_259Health Commitments and KPIs
- chap6_ul_54
- chap6_li_161Define policy/planning commitments and KPIs aligned with national strategies.
- chap6_li_162Ensure commitments demonstrate additionality and can be monitored and verified.
- chap6_li_163Draft and negotiate a commitment agreement, linking non-performance to financial penalties or default triggers.
- chap6_li_164Arrange for independent verification and reporting (define scope, frequency, costs).
260chap6_p_2609
261chap6_p_261Approvals, Legal Opinions and KYC
- chap6_ul_55
- chap6_li_165Obtain all government approvals (Parliament, Cabinet).
- chap6_li_166Secure approvals from credit enhancers and arrangers.
- chap6_li_167Obtain legal opinions from the Attorney General’s Office or equivalent.
- chap6_li_168Complete KYC requirements for all parties early to avoid delays.
262chap6_p_26210
263chap6_p_263Account Setup and Funds Flow
- chap6_ul_56
- chap6_li_169Identify and open required bank accounts (onshore/offshore).
- chap6_li_170Finalise funds flow statement and sign related letters of instruction.
- chap6_li_171Ensure mechanisms are in place for disbursement, tender payments and savings transfers.
264chap6_p_264
265chap6_p_26511
266chap6_p_266Execution, Monitoring and Reporting
- chap6_ul_57
- chap6_li_172Execute tender and new financing transactions.
- chap6_li_173Issue new loan/bond and retire old bonds.
- chap6_li_174Transfer and allocate savings as agreed.
- chap6_li_175Maintain confidentiality and communication discipline until closing.
- chap6_li_176Implement monitoring and third-party verification of KPIs.
267chap6_p_26712
268chap6_p_268Post-Closing Follow-Up
- chap6_ul_58
- chap6_li_177Begin regular reporting to partners, credit enhancers and investors.
- chap6_li_178Review compliance with KPIs and covenant performance.
- chap6_li_179Manage ongoing relationships with trust fund, DFIs and verification agents.
- chap6_li_180Document lessons learned for future transactions.
Chapter 7: The Use of Public-Private Partnerships in Healthcare Projects
Key Takeaways
|
|
1chap7_p_1This chapter, presented in two parts, provides a comprehensive overview of PPPs in the health sector. Part 1 explores the foundational aspects of health PPPs, beginning with an explanation of what PPPs are and the benefits they can bring to healthcare delivery. It examines the enabling conditions that contribute to successful implementation, compares traditional procurement methods with PPP approaches, and outlines the different types of health PPPs and their financing considerations. The section also emphasises the importance of effective stakeholder management in achieving project objectives.
2chap7_p_2Part 2 builds on this foundation by focusing on the practical dimensions of developing and managing health PPP projects. It provides technical guidance to the team designing and implementing the health PPP project. Specifically, it discusses how to build a pipeline of viable PPP projects, prepare and structure them for procurement, allocate risks appropriately and select suitable contractual models. The section concludes with guidance on the key contracts used by procuring entities and best practices for managing PPP contracts over their lifecycle.
Part 1: Understanding Health Public-Private Partnerships
Description and Rationale
3chap7_p_3PPPs are a globally recognised method of procurement. There is no single, internationally accepted definition of PPPs, but broadly speaking, a PPP can be defined as:
4chap7_p_4“A long-term contract between a private party and a procuring entity, for the provision of a public asset and/or service, in which the private party bears significant risk and management responsibility, and where remuneration is linked to performance.”
5chap7_p_5Procuring entities can include central government ministries, state departments, state agencies, state-owned entities and municipal entities. In a healthcare context, these entities typically include the Ministry of Health (MoH), health boards and hospital trusts (or equivalent entities), among others.
6chap7_p_6The duration of a PPP contract is typically between 10 and 30 years, allowing sufficient time for the asset to be affordable on an annual basis. However, the duration of a PPP contract can be shorter (e.g. for a service-only contract or digital health technologies) or longer (e.g. larger-scale projects where the private provider needs longer to recoup its investment).
7chap7_p_7Some key considerations related to PPPs include:
- chap7_ul_2
- chap7_li_10The functions for which the private party is responsible vary, but may include design, construction, renovation, financing, maintenance and operation.
- chap7_ul_3
- chap7_li_11PPP projects often involve the procurement of new assets; however, some PPP arrangements also involve the rehabilitation and/or maintenance of existing assets.
- chap7_ul_4
- chap7_li_12Risks are allocated to the party best able to bear them.
- chap7_ul_5
- chap7_li_13Each of the phases of the PPP project is generally addressed in one contract (e.g. a project agreement or concession agreement).
- chap7_ul_6
- chap7_li_14The private party typically operates through a special purpose vehicle (SPV), a separate, legally independent company that is created to carry out a specific project.
- chap7_ul_7
- chap7_li_15The payment mechanism in a PPP contract may include a tariff or user fee model, an availability-based model or a combination of these, with or without a subsidy. There will also typically be a performance management system with key performance indicators (KPIs) and a payment deduction mechanism.
- chap7_ul_8
- chap7_li_16PPPs can be applied across different sectors (including the health sector), but there might be some government limitations (e.g. some countries cannot have PPPs in the defence sector).
Rationale
8chap7_p_8PPPs can be an effective way of supporting UHC as they mobilise private sector financing and expertise, which can close the funding gap while bringing efficiencies into health systems. Governments should be clear on the issues they are seeking to solve by involving the private sector in healthcare delivery. This can take several forms or a combination thereof:
- chap7_ul_9
- chap7_li_17Closing the infrastructure gap. Through PPPs, governments can accelerate the delivery of infrastructure needed for a range of facilities such as clinics, hospitals and diagnostic centres without bearing the full upfront fiscal burden, while ensuring long-term performance and service quality through outcome-based partnership contracts.
- chap7_li_18Closing the medical equipment gap. PPPs enable access to medical technologies through various mechanisms, including leasing, build-operate-transfer (BOT) and managed equipment service (MES) models that improve clinical outcomes and operational efficiency. By aligning incentives between public health objectives and private sector innovation, PPPs help strengthen resilience, expand access to care and modernise health systems in a financially sustainable and scalable way.
- chap7_li_19Dealing with shortages in healthcare workers and specific skill sets. The shortage in healthcare workers (HCWs) and specialised skills is a significant global challenge. These issues are most profound in low and middle-income countries, particularly in Africa, which has 25% of the world’s disease burden but has only 3% of global HCWs. PPPs can work towards increasing the employment and utilisation of HCWs in Africa by providing additional employment opportunities, focusing on training and professional development, particularly in areas where there is a shortage of specialists, improving retention and optimising the utilisation of HCWs. Moreover, the private sector can leverage medical equipment, digital health technologies and artificial intelligence to enable healthcare delivery in resource-scarce environments.
Case Study: Applicability of PPP in the Improvement of Clinical Services and Renovation of Existing Facilities9chap7_p_9The Ministry of Public Health had received a public hospital from a donor but was unable to operate the hospital to acceptable clinical standards. The need to improve clinical services, as well as renovate the existing facilities and develop a new pharmaceuticals facility, led the Ministry to explore the possibility of harnessing private sector investment and managerial skills for the hospital. The Ministry outlined its requirements for the core clinical services to be provided to patients, including maternity health services, neonatology services, paediatric health services, oncology, medical, surgical and radiotherapy services, as well as diagnostic services. A key consideration was the patient mix, ensuring that not only private patients but also a percentage of low-income patients could access the enhanced facilities at no cost. |
- chap7_ul_10
- chap7_li_20Improving operational efficiency and realising cost savings. PPPs can improve operational efficiency and realise cost savings in healthcare systems by introducing private sector innovation, management expertise and performance-driven accountability into the delivery of healthcare services. Through well-structured PPP contracts, the public sector can shift from input-based spending to outcome-based models (value-based healthcare) that reward efficiency, quality and patient satisfaction. The private sector’s ability to optimise workflows, deploy digital health solutions and implement preventive maintenance systems can reduce inefficiencies in hospital operations. Economies of scale can be achieved through integrated procurement, supply chain management and shared service models. The public partner must be able to meet its payment obligations and monitor outcomes and KPIs.
Enabling Conditions
10chap7_p_10To incentivise investments in healthcare PPP projects, countries need a transparent, stable and predictable investment ecosystem that allows for transparent and efficient contracting processes and contract enforcement. This needs to be underpinned by sound health policies and embedded into institutions that enable the private sector, both domestic and international, to operate efficiently, profitably and with maximum development impact. Therefore, promoting and protecting health-related investments requires special emphasis from governments to ensure that appropriate regulatory and policy frameworks are in place.
11chap7_p_11Potential investors will assess the domestic legal and regulatory environment in the relevant country before deciding to participate in any healthcare PPP project. Each country will have their own legal and regulatory considerations and risks, which will naturally impact the nature and extent of any investment that may be provided for a specific healthcare PPP project. Any such assessment will need to be carried out by potential investors on a case-by-case basis, and each investor will have their own particular requirements that must be satisfied before any investment is contemplated.
12chap7_p_12A list of the common issues or risks that need to be considered by investors as part of their country due diligence before investing in health PPP projects includes:
- chap7_ul_11
- chap7_li_21The rule of law is a fundamental pillar and indicator of a country’s readiness for investment. Linking to a variety of risk categories, including a country’s legal and regulatory environment, control of crime and corruption, and disputes, the rule of law underpins the legal certainty in and of a jurisdiction.
- chap7_li_22The legal and regulatory environment allows investments (foreign direct investment limits, bankruptcy and insolvency laws and investment and assurance laws).
- chap7_li_23The availability of international arbitration as a dispute resolution mechanism.
13chap7_p_13There should be a solid legal framework which clearly applies to health PPP projects. A critical part of this framework is having a robust PPP law. The key requirements for an effective PPP law include:
- chap7_ul_12
- chap7_li_24Harmonisation of the institutional framework for the implementation of PPP projects, which would apply to health projects.
- chap7_li_25Enabling the participation of the private sector in the development and implementation of PPP projects, including through the incentivisation of public/private collaboration.
- chap7_li_26Provision for clear procurement procedures, including guidelines on competitive procedure and the unsolicited procedure.
- chap7_li_27Identification of the types of state support which may be available for health PPP projects on a case-by-case basis, such as sovereign guarantees and undertakings, viability gap financing, subsidies, tax exemptions and/or benefits (See also Chapter 8: Credit Enhancement).
Challenges
14chap7_p_14In Table 7.1 below, we have identified a selection of typical challenges that can adversely affect the implementation of health PPPs, along with suggested solutions for each challenge.
|
15chap7_p_15Typical Challenge |
16chap7_p_16Solution |
|
17chap7_p_17Inadequate legal framework, policies and enforcement |
18chap7_p_18There should be a solid legal, policy and regulatory framework which clearly applies to health PPP projects. This should include laws relating to PPP, procurement, investment and private sector participation in healthcare. 19chap7_p_19A robust institutional framework is usually best enforced through a central PPP unit, typically housed within the Ministry of Finance (MoF). |
|
20chap7_p_20Lack of prioritisation within government ministries or interference from government ministers which can lead to delays. 21chap7_p_21 |
22chap7_p_22There should be political will to support health PPPs and ongoing political stability. Long-term health PPP projects need appropriate long-term support. To avoid interference, proper governance and approvals procedures should be introduced and consistently applied. |
|
23chap7_p_23A weak payment mechanism for remunerating the private partner (e.g. public and/or mandatory private health insurance or inadequate remuneration levels). |
24chap7_p_24This does not enable payments to be output-based. While it does not prevent PPP schemes from proceeding, the payment mechanism will be based on cost reimbursement and a margin. |
|
25chap7_p_25Lack of capacity and capability among government officials. 26chap7_p_26 |
27chap7_p_27A programme of health PPP capacity building should be introduced to ensure that there are trained and experienced public sector personnel, focused on delivery. |
|
28chap7_p_28Lack of interest from tenderers, possibly due to a lack of knowledge about the jurisdiction and publicity about the health PPP programmes/projects. |
29chap7_p_29The procuring entity should publish a visible and credible pipeline of health PPP projects. It is recommended that the procuring entity carry out preliminary market engagement with the private sector market and understand what might be the competing projects to their health PPP programme. |
|
30chap7_p_30Poor contract packaging occurs when PPP contracts are too small, too diverse or too risky. 31chap7_p_31 |
32chap7_p_32The procuring entity should undertake comprehensive feasibility studies and business cases as part of preparing the PPP project. Bundling projects together or separating them into parts may be advisable to match the scope that the market is ready to undertake. |
|
33chap7_p_33Inappropriate or unrealistic risk transfer, for example, occurs when all risks are fully allocated to the private partner. |
34chap7_p_34The procuring entity should undertake a full risk assessment of the proposed PPP project. |
|
35chap7_p_35Failure to comply with and/or apply health PPP contractual provisions, which can result in delays, disputes, fraud and corruption. |
36chap7_p_36The procuring entity should undertake robust contract administration. |
|
37chap7_p_37Failure to establish strong stakeholder arrangements. |
38chap7_p_38It is essential to engage all necessary stakeholders and manage their expectations, and to spend time planning and managing both the development and implementation of the health PPP. |
|
39chap7_p_39Relegation of sustainability considerations |
40chap7_p_40Environmental, social and governance (ESG) principles align closely with public health objectives - reducing waste, improving working conditions and ensuring equitable access to care. ESG considerations should be built into health PPP procurement and operation (e.g. sustainable hospital design or climate-resilient infrastructure). |
Types of Health PPPs
41chap7_p_41Health projects can be procured in several ways, ranging from full public delivery to arrangements where private partners are responsible for ongoing service provision. This chapter focuses on PPPs where the private partner contributes private finance and delivers the project. The chapter does not include engineering, procurement and construction (EPC) projects where the private provider does not provide an ongoing service after the completion of the construction phase.
42chap7_p_42Figure 7.1 illustrates the continuum of procurement from fully public to PPP models. This section elaborates on how PPP models, shown at the latter end of this spectrum, are used to deliver specific activities in the health sector.
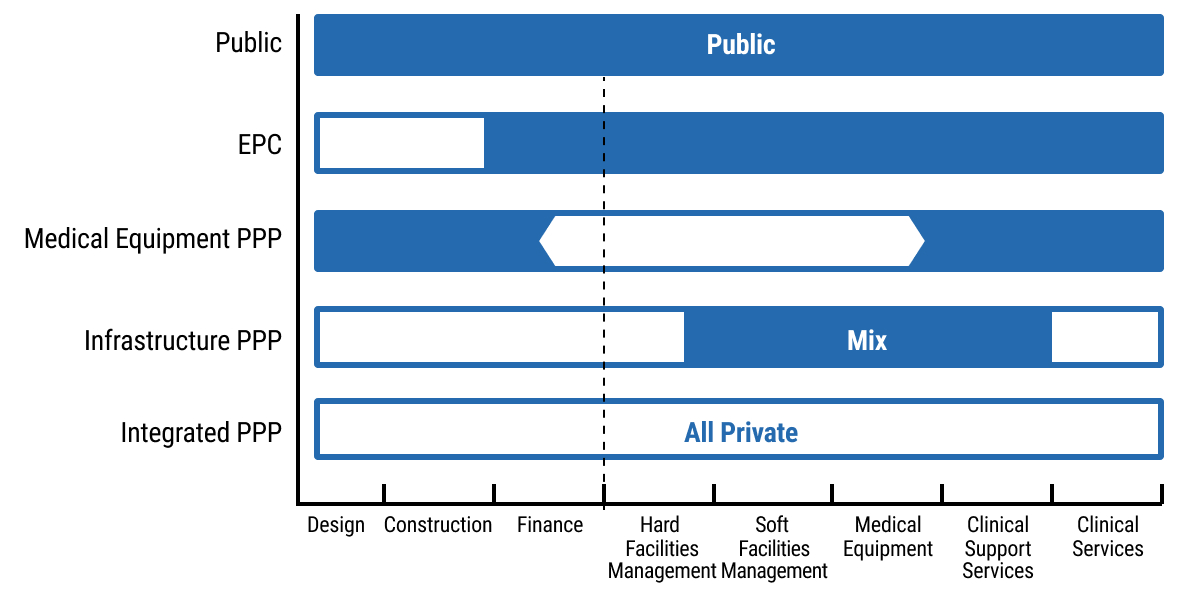 chap7_img_0
chap7_img_0
43chap7_p_43Various types of PPPs are described briefly below.
Infrastructure PPPs
44chap7_p_44In infrastructure PPPs, the private partner undertakes the planning, design, construction, equipping, financing, facilities management and non-clinical services while the public partner is responsible for the clinical services. This method has been widely adopted in the U.K., Canada, Australia, Europe and recently in Saudi Arabia.
45chap7_p_45The diagram below presents a simple organisation chart showing how the parties in an infrastructure PPP are interrelated. The private partner is shown as an SPV, which enters into the PPP agreement with the procuring entity (shown as the Public Partner) and receives payment from the public partner in the form of an availability payment (a payment made once the asset is available for use per the contract). The funding comes primarily from the sponsor (or investor) as equity and from the lender as debt. The SPV then enters into subcontract arrangements for the design and build of the facility, for providing and installing medical equipment, and for undertaking facilities management.
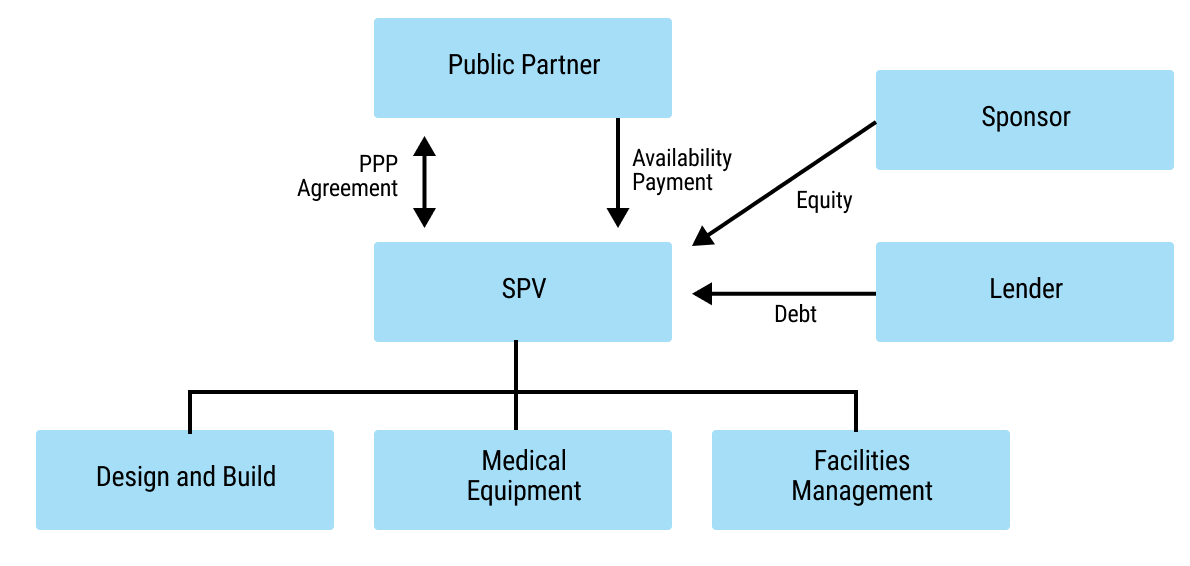 chap7_img_1
chap7_img_1
46chap7_p_46Infrastructure PPPs typically have long tenors of 20-30 years, and require financing with favourable terms to keep the cost of capital affordable.
47chap7_p_47The private partner typically receives an availability payment for making the asset available and a service payment for providing the non-clinical services.
48chap7_p_48The hospital’s capacity is planned to meet the public sector’s requirements, often leaving limited scope for optimising the design and operations. This model is attractive to funders and investors as it carries no demand risk. The private partner’s key risks are the completion of the development works on time and meeting the availability criteria, as well as ensuring the facility meets its key performance requirements.
49chap7_p_49The PPP can additionally help incentivise efficiencies within the private partner. For example, the private partner could be responsible for energy and water consumption costs at a set tariff. This shares the risk between the public and private partners, with the private partner designing and building energy-efficient buildings and the public provider incurring the risk if the tariff rate increases.
Case Study: Private Sector Innovation Through a New Health PPP Model in the U.K.50chap7_p_50The New Velindre Cancer Centre (nVCC) is one of three Welsh Government pilot projects and the first hospital to use the new Mutual Investment Model (MIM). This model includes a 15% public sector stake in the SPV and a significant community benefits package mandated through procurement. Key innovations include:
|
Medical Equipment PPPs
51chap7_p_51Similar to infrastructure PPPs, in the medical equipment PPP model, the private partner undertakes the planning, design, equipping, and, if needed, any construction or retrofitting. In addition, the private partner finances the project and undertakes the maintenance and any facilities management services associated with the medical equipment and its surroundings.
52chap7_p_52There are two options for operating the medical equipment itself:
- chap7_ul_14
- chap7_li_31By the public partner, in which case the model is akin to an infrastructure PPP.
- chap7_li_32By the private partner, where the public partner would be required to agree on the diagnostic service volumes and agree to a set of tariffs.
53chap7_p_53
54chap7_p_54This PPP type typically has shorter tenures of 7-12 years, which is compatible with the life cycle of the equipment.
Case Study: Managed Equipment Services (MES) in Kenya55chap7_p_55The Kenyan government entered into contracts with several original equipment manufacturers (OEMs) to enhance access to and equity in healthcare. Under the MES arrangement, OEMs were responsible for supplying, installing, maintaining and replacing medical equipment, as well as providing user training across hospitals nationwide. 56chap7_p_56The MES programme was successfully implemented, significantly upgrading specialised health infrastructure and expanding access to critical healthcare services nationwide. Previously unavailable services, such as dialysis, critical care, surgical theatres, sterilisation and advanced imaging, were introduced or expanded in multiple hospitals. 57chap7_p_57The programme ensured reliable equipment installation and maintenance, enhanced the capacity of healthcare workers (HCWs) through training and fostered a more enabling work environment. Key lessons learned included the importance of: (i) defining detailed equipment specifications, (ii) ensuring comprehensive stakeholder engagement, and (iii) allocating sufficient time for assessment, procurement, and implementation. |
Digital health PPPs
58chap7_p_58Digital health PPPs support the transformation of healthcare businesses and sector-wide processes and operations by adopting digital technology, creating new opportunities and driving change. PPPs in digital health typically require combining the agility of the private sector with public sector access to patients and medical records. They tend to have even shorter tenors, given the short lifespan of these technologies. These partnerships rely on speedy implementations of ready solutions or those at the beta test stage.
59chap7_p_59
Case Study: Digital Health - Estonia, Electronic Health Record60chap7_p_60Estonia’s journey towards digital healthcare has involved collaboration between the government and various technology providers to develop, implement and manage its national electronic health record (EHR) and e-Health systems. While the specific details of the agreements and partnerships that facilitated the rollout of Estonia’s EHR system may vary and involve multiple contracts and collaborations, the overarching strategy aligns with the PPP model. This model leverages both public oversight and governance, as well as private sector innovation and efficiency, to achieve public health goals. Its digital health ecosystem, known for its e-Health Record system, integrates data from various healthcare providers, providing patients and doctors with online access to medical histories, prescription information and test results. 61chap7_p_61This initiative has significantly enhanced the efficiency of healthcare delivery, improved patient safety and strengthened data security. According to the Estonian e-Health Foundation, the system has led to a 30% reduction in duplicate testing, saving time and resources. |
Case Study: Artificial Intelligence - United Kingdom, Google and the National Health Service62chap7_p_62The collaboration between Google’s DeepMind and the U.K.’s National Health Service on improving eye disease detection through AI technology exemplifies successful PPPs in healthcare. This project utilised AI to analyse eye scans for conditions such as diabetic retinopathy and age-related macular degeneration, which specialists traditionally diagnose. By leveraging DeepMind’s artificial intelligence to interpret optical coherence tomography (OCT) scans, the partnership aimed to enhance diagnostic speed and accuracy. Trained on a vast dataset of de-identified OCT scans from Moorfields Eye Hospital, the AI system matched the accuracy of leading experts in identifying eye diseases. This collaboration enhanced diagnostic efficiency, alleviated specialists’ workload through automation, and demonstrated the potential for scaling AI solutions across the healthcare system. |
Training and education PPPs
63chap7_p_63Where the construction of a training institution is required, a PPP could be used, similar to infrastructure PPPs. This could be extended to a model where the private partner provides the facilities and pedagogical services (I.e. gives pre-service training to HCWs).
Private Wings in Public Facilities
64chap7_p_64Under the private wings in the public facilities model, a public hospital enters into an arrangement with a private partner to establish a private patients’ wing on its premises. In that case, the private partner attracts private paying patients and admits them to that wing, providing all the hotel services (e.g. catering) while utilising the diagnostic and treatment services offered at the hospital to public patients. This arrangement typically takes the form of a lease or sublease of the private patient wing, with admission rights granted and a service level agreement (SLA) in place for the services provided by the public hospital. The SLA specifies matters such as response times, prices, risk and liability.
Case Study: Expansion of Commercial Activities at a Public Hospital65chap7_p_65A public hospital in the U.K. had already expanded its commercial activities with the objective of cross-subsidising the costs of public healthcare. As part of its commercial strategy, the public hospital assessed the potential to further increase the profitability of its private patient income, generating additional funds to reinvest in public hospital services. The benefits of using the Private Patient Admissions model included:
66chap7_p_66 |
Integrated PPPs
67chap7_p_67The Integrated PPP model involves comprehensive outsourcing, whereby planning, design, construction, equipping, staffing, financing, operations and management are outsourced on a long-term contract basis to a private partner. This PPP type introduces significant efficiencies into the operations as the contracting is based on a set of clinical activities, not based on capacity parameters - such as bed count - (as is the case with infrastructure PPPs).
68chap7_p_68The diagram below provides a simple organisation chart showing how the parties in an integrated PPP are interrelated. The private partner is shown as an SPV, which enters into the PPP agreement with the public partner and receives payment from the public partner in the form of an availability payment. In addition, the SPV receives payment for clinical services provided to patients, typically from the payer system (e.g. the public partner or national health insurance scheme). The funding it receives comes primarily from the investor (or sponsor) as equity and from the lender as debt. The SPV then enters into subcontract arrangements for the design and build of the facility, for providing and installing medical equipment and for undertaking facilities management. Importantly, the SPV is responsible for all the inputs required to deliver clinical services to patients, including hiring staff and procuring all necessary consumables.
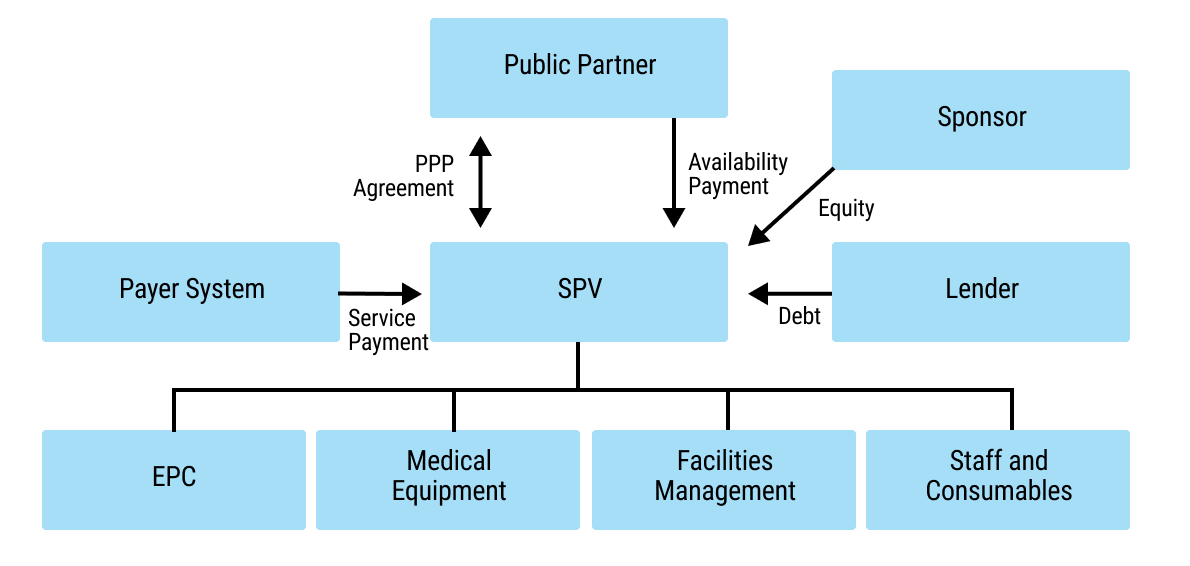 chap7_img_2
chap7_img_2
69chap7_p_69The payment mechanism can be calculated based on the catchment population (I.e. a capitation system) or using a fee-for-service model (e.g. using diagnostic-related groups), or a combination of both.
Case Study: La Ribera Hospital, Valencia, Spain70chap7_p_70This PPP combined the development and operation of a 300-bed hospital with four integrated healthcare centres and 46 public primary care centres, covering a catchment population of 250,000 people in the Alzira region. The project was structured as a 15-year concession (5-year extension option) with payment on a capitation basis. Payment covered the entire care continuum for patients, which incentivised the provider to encourage the population to undergo screening, preventative and awareness programmes. 71chap7_p_71This resulted in improved patient satisfaction and increased efficiency, with shorter waiting lists, lower lengths of stay and higher utilisation of surgical theatres. |
Case Study: Managing Capacity Constraints in a Health Sector PPP72chap7_p_72A major healthcare PPP in a lower-income country illustrated that, while such arrangements can improve healthcare infrastructure and service delivery, strong government capacity and effective contract management are critical for success. The project, which replaced a national referral hospital and introduced new clinical services, initially achieved higher-quality care and efficiency. 73chap7_p_73However, costs escalated dramatically due to weak oversight, unclear risk allocation and inadequate financial controls, consuming an unsustainable share of the national health budget. The main lesson learned is that PPPs in social sectors such as health require robust institutional capacity, transparent monitoring and flexibility to adjust terms over time to prevent fiscal strain and ensure long-term sustainability. |
Management Contracts
74chap7_p_74The management contracts PPP model is used in countries where there is insufficient capacity in the public system and/or resources to operate its hospitals. In such cases, a facility would be built, and then a private operator would be brought in to commission and manage it.
Purchasing Services
75chap7_p_75Under a purchasing services model, the public health system purchases specific procedures from the private sector, such as dialysis, diagnostics, angiograms and certain surgeries.
Financing Considerations
76chap7_p_76PPP projects are typically financed using a range of financial instruments, each bearing a level of risk and attracting a certain cost of capital. By allocating different levels of risk across the capital structure, it is possible to have a more acceptable weighted average cost of capital (WACC). Typical instruments found across the capital structure are listed below (in decreasing order of risk):
- chap7_ul_16
- chap7_li_38Equity. This is the capital invested by the private partner to own the project (or part thereof), taking on the highest risk but also receiving the highest potential return. Unlike investors in debt instruments, equity investors are owners with a stake in the project’s success and are liable for any initial losses.
- chap7_li_39Quasi-equity. This type of financing falls between a traditional loan and an equity investment. It behaves somewhat like shares - because the investor can earn a higher return and, in some cases, the loan can later be converted into an ownership stake - but it does not give the investor control or equity from the outset. It is sometimes referred to as mezzanine or subordinated debt. Because it carries more risk than a standard loan, the investor receives a higher, fixed return (similar to a guaranteed dividend). This kind of capital can help make a health PPP viable by filling the gap between regular bank loans and full equity investment.
- chap7_li_40Senior debt. This refers to the debt that takes priority over other types of financing, in the event of a default or liquidation. It is typically the first to be repaid before others in the capital structure. In PPPs, senior debt is usually provided by banks or other financial institutions and is secured against the project’s assets and proceeds, ensuring a lower risk for the lenders. Senior debt can also be arranged as a bond issue. See also Chapter 5: Sustainable Finance Instruments for a description of bonds and loans. Given its priority, senior debt often comes with lower interest rates compared to junior debt. A key component in the financing structure of PPP projects is providing funding for the initial capital investment required for infrastructure projects.
77chap7_p_77An essential aspect of making healthcare projects more affordable and sustainable is to introduce efficiencies in the design and delivery of the infrastructure and remove unnecessary costs in service delivery. However, in the context of a PPP, it is also essential to lower the WACC of the project by:
- chap7_ul_17
- chap7_li_41Maximising the amount of senior debt.
- chap7_li_42Lowering the cost of senior debt.
- chap7_li_43Lowering the cost of equity by introducing quasi-equity instruments to the extent permissible under the PPP law or the PPP agreement.
- chap7_li_44Utilising viability gap funding in one or more of the forms listed below, and blending them with equity and, as required, quasi-equity and senior debt. This serves as a form of credit enhancement (see Chapter 8: Credit Enhancement for more details). This mechanism is referred to as blended finance and could leverage:
- chap7_li_45Grant funding that could be provided by the public sector or by donor partners.
- chap7_li_46Concessional loans, supplied by development finance institutions (DFIs) or multilateral development banks (MDBs).
- chap7_li_47Debt-for-health swaps (see Chapter 6: Debt-for-Health Swaps) could generate financial flows over time to enhance the PPP financing structure.
- chap7_ul_18
78chap7_p_78To maintain the oversight and governance structure that can be required to manage blended finance resources, special trust funds may be set up for disbursing the funds and overseeing the achievement of the applicable health programme and/or KPIs.
79chap7_p_79Channelling blended finance into PPP projects comes with the benefit of financial sustainability. These additional resources will lower the WACC, making the project more affordable to the government and/or to users.
80chap7_p_80Beyond the mobilisation of financing instruments, there are key financial considerations that are inherent to the PPP project, some of which have already been mentioned in the section above on Enabling Conditions:
- chap7_ul_19
- chap7_li_48Demand risk. The extent to which demand risk is transferred to the private partner in the first place. If demand risk is transferred, whether this is accompanied by a minimum patient volume guarantee, such that utilisation rates are predictable and sufficient to ensure revenue stability for the private partner.
- chap7_li_49Payment mechanism. Clarity and reliability of how the private party is paid (e.g. availability payments, service fees, user tariffs or combination thereof).
- chap7_li_50Government support. Extent and enforceability of guarantees, subsidies or minimum revenue undertakings to enhance financial confidence.
- chap7_li_51Creditworthiness of offtaker. The financial health and payment history of the government or public entity making payments.
- chap7_li_52Tariff or fee setting. Establishing a tariff in the first place, and if so, the ability to adjust tariffs or payments in line with inflation, cost changes or performance targets.
- chap7_li_53Project preparation. Quality of feasibility studies, demand forecasts and risk allocation frameworks underpinning the project.
- chap7_li_54Regulatory environment. Clarity, predictability and stability of healthcare and PPP regulations affecting licensing, pricing and service delivery.
- chap7_li_55Political and policy stability. Government commitment to the PPP structure and avoidance of arbitrary policy changes.
- chap7_li_56Risk allocation. Appropriate distribution of construction, demand, operational and regulatory risks between public and private parties.
- chap7_li_57Land and site issues. Secure access to the project site, clear title and timely availability of utilities and supporting infrastructure.
- chap7_li_58Approvals and licensing. Streamlined processes for health facility accreditation, environmental and operational approvals.
- chap7_li_59Performance standards. Precise service level requirements and measurable KPIs linked to payments.
- chap7_li_60Termination regime. Fair compensation framework in the event of early termination due to government or private default.
- chap7_li_61Step-in rights. The right of lenders to step in and cure defaults before termination to protect their interests.
- chap7_li_62Currency and forex risk. Mechanisms to mitigate foreign exchange volatility where financing is in hard currency but revenues are local.
- chap7_li_63Dispute resolution. Efficient, neutral and enforceable mechanisms (e.g. arbitration) for resolving contractual disputes.
- chap7_li_64ESG and social impact. Compliance with environmental, social and governance standards and alignment with public health goals.
- chap7_li_65Capacity of public counterparty. Institutional ability to manage and monitor complex PPP contracts over the project lifecycle.
- chap7_li_66Bankable documentation. Well-drafted concession, project and finance agreements that align with lender requirements.
Stakeholder Management
81chap7_p_81Health PPPs bring together diverse actors drawn from government agencies, financiers, developers, operators, healthcare professionals and communities. The success or failure of these partnerships often hinges on how stakeholders are identified, engaged and managed throughout the PPP lifecycle. This section explores the critical role of stakeholders in health PPPs, emphasising stakeholder management, cross-governmental collaboration and best practices that drive successful project outcomes.
82chap7_p_82The first step involves mapping the stakeholder landscape in health PPPs to identify who matters most, their level of influence and potential risks associated with ignoring their interests. The typical players who are engaged in health PPPs are:
- chap7_ul_20
- chap7_li_67Public Sector Stakeholders such as the MoH, MoF, PPP units and procuring entities (also known as contracting authorities) and regulators.
- chap7_li_68Private Sector Stakeholders such as developers and investors, operators and facility managers, contractors and suppliers, health professionals and institutions, professional associations and unions.
- chap7_li_69Other stakeholders include development partners, donors, communities and civil society more broadly.
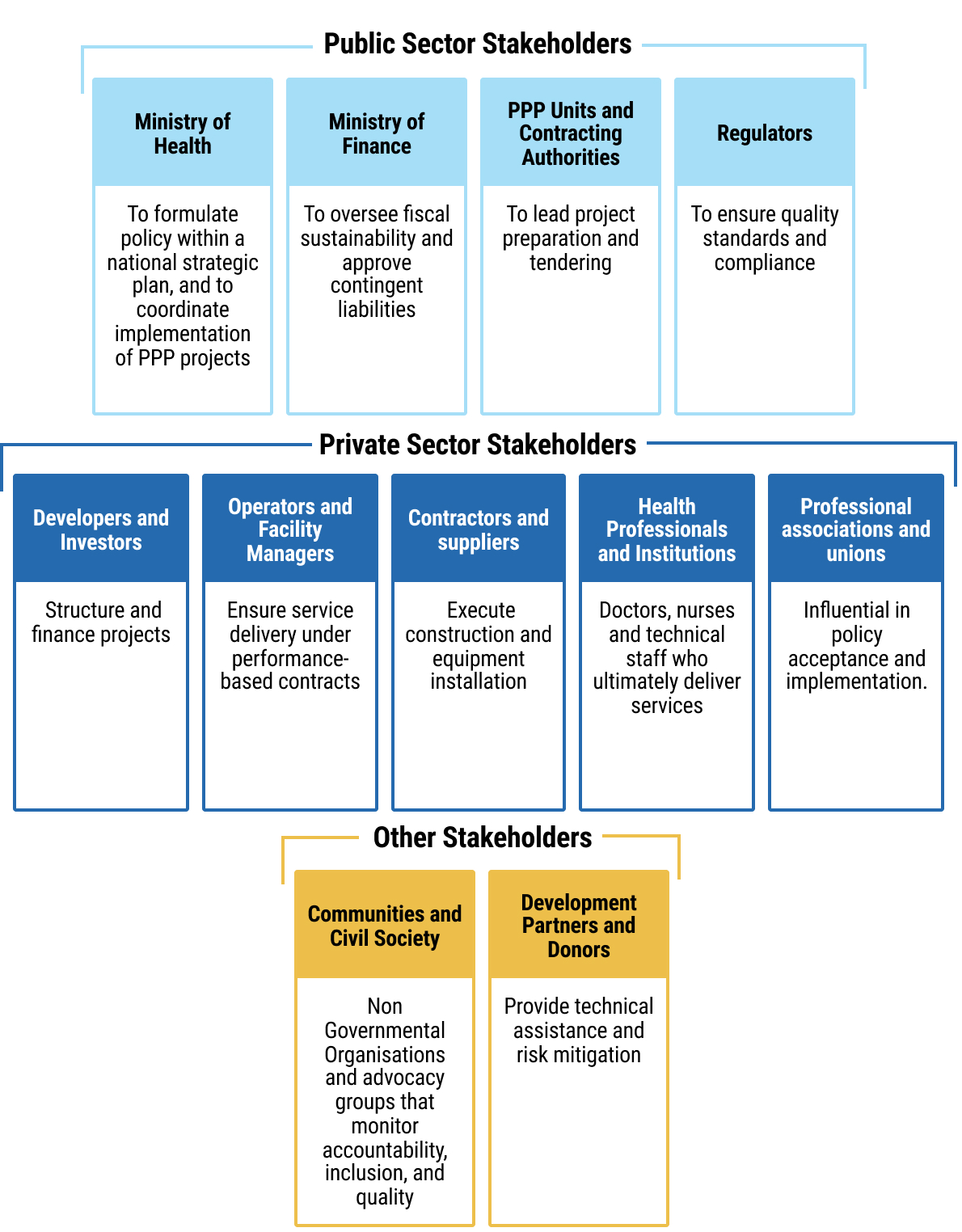 chap7_img_3
chap7_img_383chap7_p_83The second step is stakeholder management, a strategic process that ensures alignment, communication and collaboration among actors with differing interests. The four pillars of stakeholder management consist of identification, analysis, engagement and monitoring/feedback:
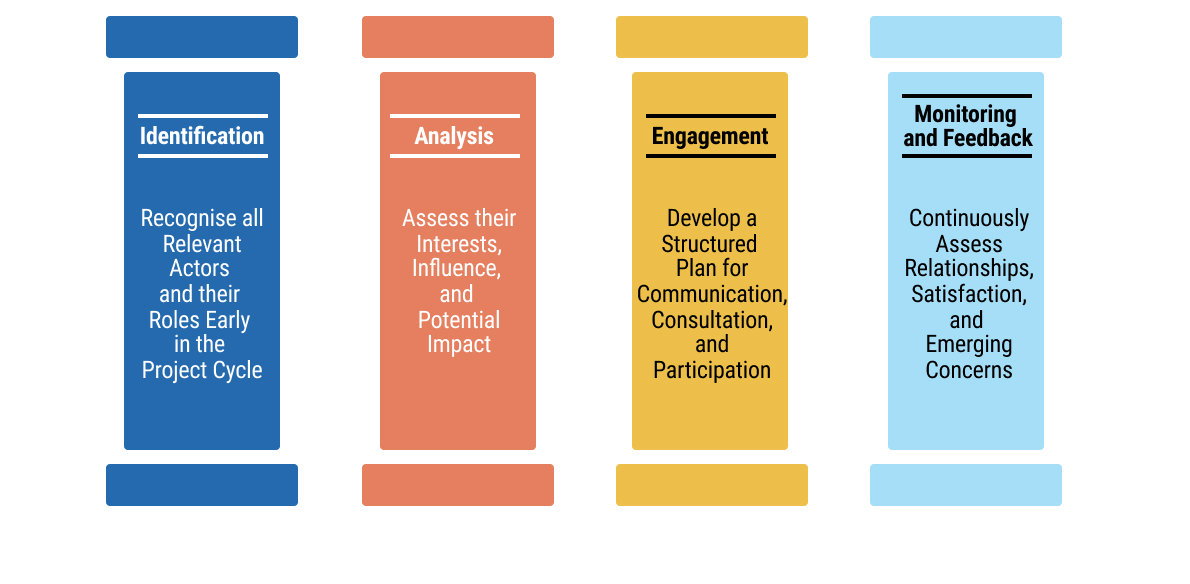 chap7_img_4
chap7_img_4
84chap7_p_84Common challenges in stakeholder engagement include:
- chap7_ul_21
- chap7_li_70Asymmetric information between technical agencies and communities.
- chap7_li_71Competing priorities among ministries, e.g. the MoF and the MoH.
- chap7_li_72Limited stakeholder capacity to understand complex PPP structures.
- chap7_li_73Resistance from health workers when not adequately consulted.
85chap7_p_85
Case Study: Underestimating the Influence of Professional Stakeholders86chap7_p_86One health-sector PPP demonstrated the significant risks that can arise when stakeholder engagement is insufficient during project preparation. The initiative, aimed at enhancing service delivery through private sector participation in a major public hospital, encountered strong resistance from health professionals. Their objections stemmed from limited consultation and a lack of transparency around the proposed involvement of a private partner in managing selected clinical services within a public facility. 87chap7_p_87Health workers expressed concern that the PPP project could undermine job security, professional autonomy and the quality of patient care. The absence of structured dialogue and communication channels led to mistrust, culminating in legal action against the government. The ensuing dispute generated reputational and political risk, discouraged potential bidders, and ultimately, the project was considered for restructuring and retendering. 88chap7_p_88This case study highlights a recurring challenge in health PPPs - the underestimation of professional stakeholder influence. Health workers, as frontline service providers, hold both technical expertise and moral authority that can shape public and policy perception. Failing to meaningfully engage them early in the project cycle can therefore jeopardise project legitimacy and investor confidence. This example highlights the importance of governments establishing formal stakeholder engagement frameworks, including structured consultations with professional associations, transparent communication of project objectives and mechanisms for addressing concerns related to employment and service quality. Proactive engagement not only mitigates resistance but also builds ownership, enabling smoother implementation and greater sustainability of health PPP projects. |
Case Study: Weak Stakeholder Coordination Undermining Health PPP Implementation89chap7_p_89One health-sector PPP demonstrated how insufficient stakeholder management can compromise the effectiveness of otherwise well-structured initiatives. The partnership, intended to expand reproductive and child health services through collaboration with non-state providers, faced significant implementation challenges arising from unclear roles, weak communication and limited involvement of frontline health personnel. Divergent expectations among stakeholders, coupled with the absence of structured dialogue, contributed to mistrust, slow decision-making and uneven service delivery. 90chap7_p_90The study further revealed that local government authorities lacked the capacity and governance systems necessary to coordinate multiple actors within the partnership. Power imbalances between public and private partners, combined with inadequate monitoring mechanisms, meant that accountability was weak and collaboration often depended on personal rather than institutional relationships. This experience highlights a central lesson for health PPPs: without deliberate, well-resourced stakeholder engagement and clear governance arrangements, even promising partnerships struggle to achieve their intended impact. |
Case Study: Vietnam - The Critical Importance of Stakeholder Engagement in Health Sector Reform91chap7_p_91Vietnam’s experience with PPPs demonstrates the critical importance of stakeholder engagement in health sector reform. As the government explored converting public hospitals into PPP-operated facilities, the World Bank’s report Public-Private Partnerships for Health in Vietnam: Issues and Options found that resistance quickly emerged - not because the PPP model was technically weak, but because many stakeholders felt uninformed and uncertain. Clinicians, hospital managers and frontline workers worried about losing professional autonomy, facing new performance pressures or seeing patient care compromised by commercial priorities. 92chap7_p_92Public perception posed an equally significant barrier. Communities viewed public hospitals as social assets that should remain accessible to all. Without clear communication, many feared PPPs would lead to higher user fees or reduced access for poorer households. Political actors, sensing public unease, grew cautious about championing PPP reforms. This lack of coordinated communication created an environment where rumours and misconceptions spread faster than official information, weakening confidence in the reform process. 93chap7_p_93The Vietnam case shows that the success of PPPs depends as much on managing people, expectations and trust as it does on financial or technical design. Transparent communication, early consultation with clinicians and proactive public outreach are crucial in reducing fear and building legitimacy. The core lesson is clear: without deliberate stakeholder engagement, even well-designed PPP initiatives risk delay, opposition or failure - while effective engagement can transform reforms into shared, socially supported solutions. |
94chap7_p_94Cross-governmental collaboration is essential to deliver a PPP and ensure coherence in policy, financing and service delivery. Often, MoHs lead project design without adequate coordination with the MoF and Planning. This leads to delays, unclear mandates and inconsistent expectations. Some mechanisms could help address those coordination challenges:
- chap7_ul_22
- chap7_li_74Establishing inter-ministerial committees to align decision-making among key ministries and scoping responsibilities across agencies
- chap7_li_75Establishing a PPP committee to provide a unified project governance structure
- chap7_li_76Joint planning and budgeting to harmonise resource allocation between the MoFs and MoHs
95chap7_p_95These mechanisms could benefit from consistently applying some of the following principles:
96chap7_p_961. Engage early and continuously. Involve stakeholders from project identification through to operations. Early engagement reduces resistance and improves design relevance.
97chap7_p_972. Ensure transparency and communication. Public disclosure of project information enhances trust. Use communication plans that are proactive and multi-channel, e.g community meetings, social media and local radio.
98chap7_p_983. Institutionalise participation. Establish stakeholder advisory forums or oversight committees that meet regularly to discuss project progress and address grievances.
99chap7_p_994. Build capacity. Train both public and private actors on PPP processes, risk sharing and performance monitoring.
Part 2: The Preparation, Procurement and Delivery of Health PPP Projects
100chap7_p_100Health PPP projects generally involve high-value, complex procurements. Careful preparation and management, both before, during and after the procurement competitions, will be required to ensure the successful delivery of the health PPP project and to obtain maximum value for money.
101chap7_p_101Specific rules for structuring procurement competitions for PPP projects should be set out in a local PPP or procurement law. However, the relevant law may not foresee every eventuality that might arise during the course of a procurement competition.
102chap7_p_102Procuring entities must, therefore, exercise individual discretion in some circumstances and, in doing so, must act in accordance with the general principles of transparency, equal treatment of tenderers and taking steps which are proportionate to the outcome to be achieved.
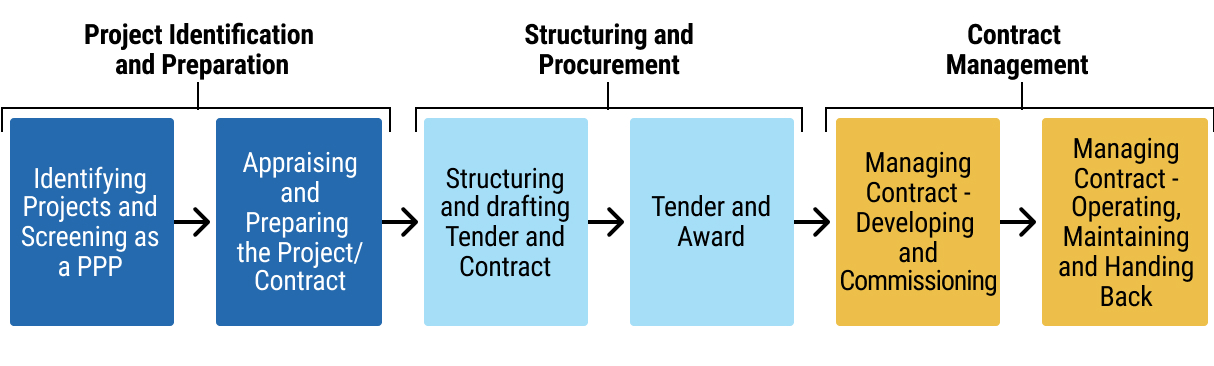 chap7_img_5
chap7_img_5
Developing a Pipeline of Health PPP Projects
103chap7_p_103To plan health PPPs effectively, the public sector first needs a clear pipeline of priority projects. This begins with a health master plan that identifies the gap between the services people need and what the system currently provides. The master plan should utilise demographic and disease-burden data - both current and projected - to determine the types of facilities required, their optimal locations and the services they should offer. These may include primary care centres, diagnostic hubs, hospitals, rehabilitation facilities and palliative care services.
104chap7_p_104The planning process should consider how to optimise operations, such as reducing lengths of stay, incentivising preventive care, shifting to outpatient settings and increasing the use of day surgeries. These improvements reduce both capital and operating costs, the latter of which typically make up most of a facility’s budget. The master plan, for example, may highlight a need for a healthcare network in a specific region that includes improved preventive care and outreach models, rather than just a new hospital.
105chap7_p_105This analysis will produce a list of potential projects that governments should prioritise based on impact, cost and feasibility. Where conditions allow, selected projects can then be developed as PPPs using appropriate PPP models.
Preparation of Health PPP Projects
106chap7_p_106Each procuring entity will need to comply with the business case approval process applicable to their health PPP project. In addition to the key decisions required as part of the business case approval process, each procurement procedure requires a considerable amount of planning and preparation by the procuring entity before a tender notice can be advertised for the health PPP project.
107chap7_p_107The readiness of each procuring entity to commence procurement will be assessed as part of the consideration of the business case for their PPP project. The issues which will be evaluated include:
- chap7_ol_0
- chap7_li_77Clear scope for the health PPP project. Have the needs and requirements of the procuring entity been determined?
- chap7_li_78Governance arrangements for the PPP project. Has governance been adequately considered and resolved? Has an accountable line of responsibility been established to which the procurement team can report? Are all the responsible players named and committed to their roles? Each health PPP project requires an appropriately skilled and experienced procurement team that leads the procurement competition, supported by informed decision-makers. The governance hierarchy for decisions to be made during the procurement competition should be circulated to all decision-makers and those involved in evaluating tenderers.
- chap7_li_79Procurement documents (including the PPP contract). How advanced is the draft documentation? Have any applicable template documents and guidance issued by the PPP unit been used, and any derogations approved? Have the risks of the health PPP project been fully identified and allocated in the PPP contract?
- chap7_li_80Appropriate market sounding. Assessing the market (for example, through market research or direct engagement with potential tenderers) to determine whether the level of private sector interest is likely to be sufficient to ensure genuine competition is crucial.
- chap7_li_81Practical matters. Have issues such as the availability of internal resources, the appointment of external advisers and the provision of electronic procurement platforms been adequately considered and resolved?
108chap7_p_108The typical procurement pitfalls set out in the diagram below must be considered and avoided (where at all possible) by the procuring entity to ensure successful procurement and implementation of their health PPP project.
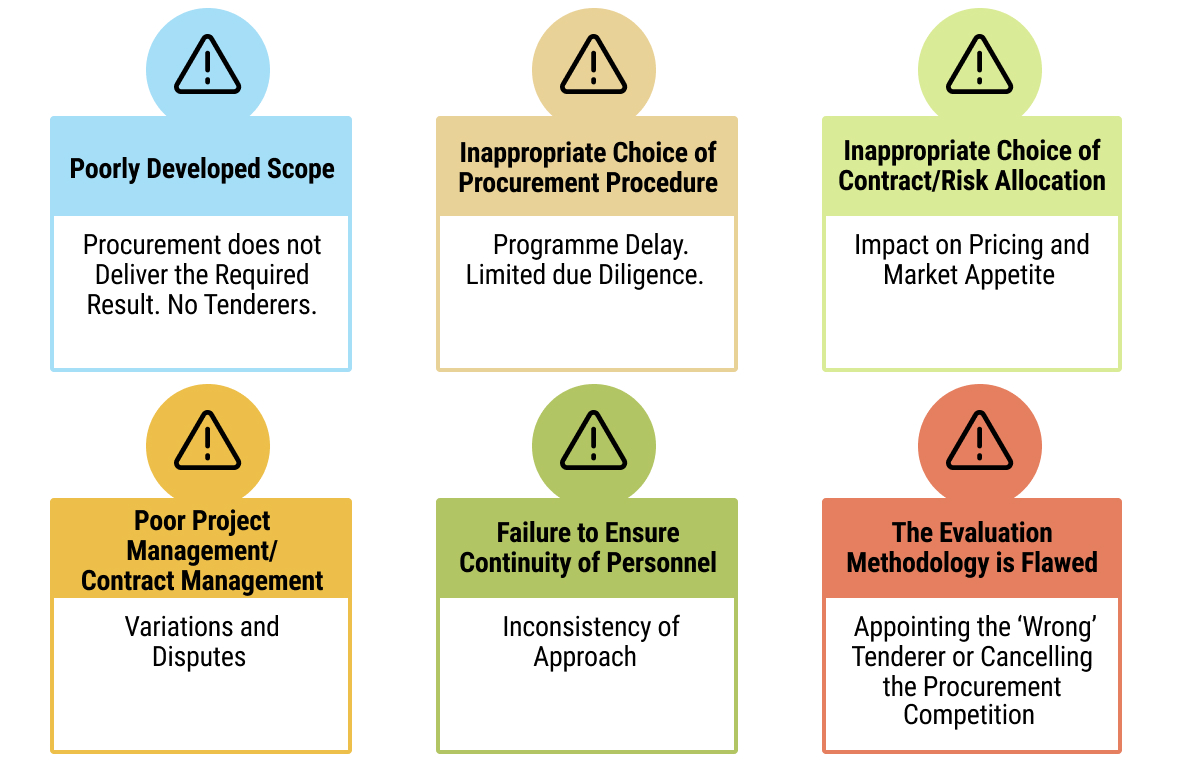 chap7_img_6
chap7_img_6
Development of the Procurement Strategy for a Health PPP Project
109chap7_p_109Several public procurement decisions will need to be made early in respect of the procurement of health PPP projects. These decisions will influence not only the structure of each procurement competition and the content of the associated tender documentation, but also market perception and the procurement timetable. In all instances, the procurement strategy must be consistent with the principles of the applicable local policy, and an appropriate procurement team, with the necessary knowledge and mandate, will have been appointed. The following key decisions are required:
The Public Procurement Procedure
110chap7_p_110In each jurisdiction, there will be various types of procurement procedures for health PPP projects, which could include the open procedure, the restricted procedure, the negotiated procedure and competitive dialogue.
111chap7_p_111Generally speaking, open procedures are unsuitable for the procurement of complex financed PPP projects as they do not allow for the shortlisting of bidders and have no mechanism for dialogue or negotiation with tenderers.
112chap7_p_112Restricted procedures are generally designed as a one-step tender process. While a shortlist of tenderers may be invited to participate (following a Request for Qualification (RfQ)), there is only one round of tenders and no mechanism for dialogue, negotiation or down-selecting after pre-qualification. This procedure would be unsuitable for the procurement of PPP projects with a complex financing structure.
113chap7_p_113The negotiated procedure or competitive dialogue permits the shortlisting of tenderers at the RfQ stage, and negotiation or dialogue during the Request for Proposals (RfP) stage. Limited negotiation and clarification is usually also permitted under the competitive dialogue procedure (following submission of final tenders). Negotiated and competitive dialogue procedures are generally more appropriate for the procurement of health PPP projects because:
- chap7_ul_23
- chap7_li_82The needs of the procuring entity cannot be met without adaptation of readily available solutions.
- chap7_li_83The PPP contract includes design or innovative solutions.
- chap7_li_84The PPP contract cannot be awarded without prior negotiation due to specific circumstances related to its nature, complexity, legal and financial makeup or because of risks attached to it.
- chap7_li_85The technical specifications cannot be established with sufficient precision by the procuring entity.
Typical Structure for a Competitive Dialogue Procurement for a Health PPP Project
114chap7_p_114It is recommended that the competitive dialogue procedure for the procurement of health PPP projects should be structured in the following successive stages:
- chap7_ul_24
- chap7_li_86Preliminary market engagement
- chap7_li_87Advertisement
- chap7_li_88Prequalification and shortlisting
- chap7_li_89RfP issued to shortlisted tenderers
- chap7_li_90Dialogue period
- chap7_li_91Close dialogue and invitation to submit final proposals
- chap7_li_92Contract award
115chap7_p_115The diagram set out below illustrates the successive stages of a typical competitive dialogue procedure for a health PPP project.
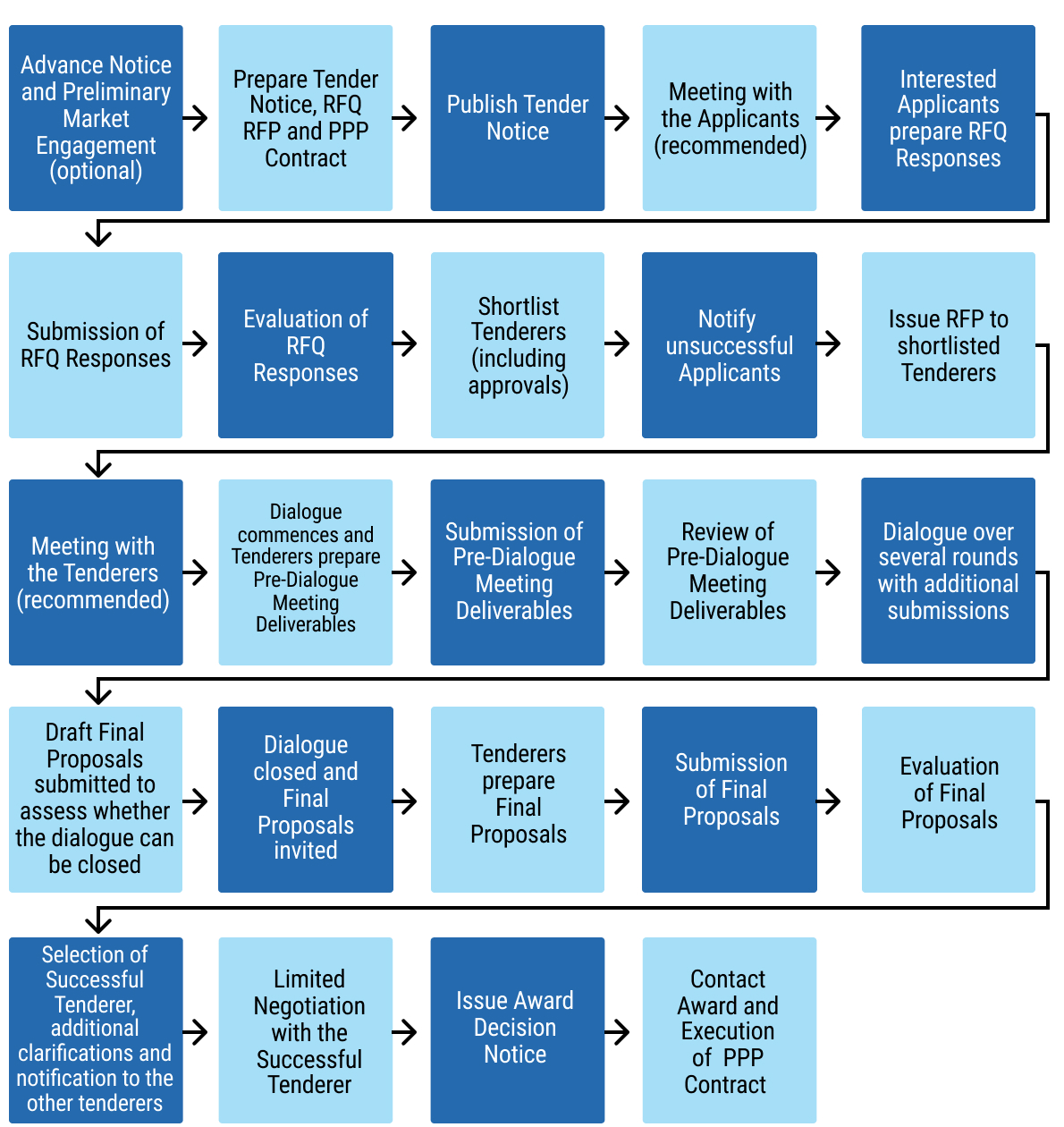 chap7_img_7
chap7_img_7
Shortlisting and Invitation of Bidders to the Procurement Competition
116chap7_p_116There will be procurement cost and time savings if fewer tenderers are shortlisted and invited to participate in the procurement competition for each health PPP project. However, there is a risk to competitive tension if fewer tenderers are shortlisted and subsequently a tenderer withdraws without submitting a final tender. It is recommended that three tenderers be shortlisted for each health PPP project. However, shortlisting more than three tenderers could be reviewed on a project-by-project basis, taking into account potential market changes.
Evaluation Criteria for Shortlisting Bidders to the Procurement Competition and Contract Award
117chap7_p_117Robust evaluation methodologies will be required for the shortlisting of bidders and the evaluation of tenders. In essence, shortlisting entails evaluating the economic and financial standing, as well as the professional/technical ability, of each bidder. Tender evaluation involves assessing the tenders received. Therefore, two sets of evaluation criteria will be required.
118chap7_p_118Tender Documents for a Health PPP Procurement Competition
119chap7_p_119There are two key tender documents for a health PPP procurement competition: the RfQ and the RfP. The purpose of the RfQ is to enable the procuring entity to identify suitably qualified and experienced tenderers who will be invited to participate in the procurement competition for the PPP project.
120chap7_p_120The RfQ should provide detailed information regarding the procuring entity’s requirements for the PPP project and arrangements. The RfQ is also an essential document for the private sector, as it enables potential tenderers to make an informed decision on whether to participate in the procurement competition.
121chap7_p_121The issue of the RfP represents a formal invitation from the procuring entity to tenderers to participate in dialogue or negotiation (where negotiated or competitive dialogue procedures are being used). The purpose of the RfP is to initiate and develop dialogue with the tenderers with a view to identifying the most advantageous tender.
122chap7_p_122The RfP should provide detailed information regarding the procuring entity’s requirements and arrangements for the conduct of the RfP stage of the procurement competition, including the submission of tenders and their evaluation.
Required Resources
123chap7_p_123Health PPP procurements require significant resourcing, both internally from the procuring entity’s personnel and externally from advisors, such as legal, financial, technical, clinical, equipment, insurance and environmental and social advisers. Roles and responsibilities for matters such as procurement, evaluation, contract negotiation and stakeholder engagement should be determined at the business case stage. A skills audit should be carried out to assess available in-house capabilities, any training requirements and the level of external support required.
Procuring Entity Project Team’s Role
124chap7_p_124Following the approval of the business case for a health PPP project, the procuring entity’s project team is responsible for:
- chap7_ul_25
- chap7_li_93Structuring the procurement competition and providing input to, and reviewing, the procurement documents (including the PPP contract).
- chap7_ul_26
- chap7_li_94Managing the RfQ process, including the clarifications process and notifying unsuccessful applicants, and evaluating RfQ responses.
- chap7_ul_27
- chap7_li_95Managing and participating in procurement competitions (including clarifications, dialogue and negotiations), and evaluating the tenders submitted.
- chap7_ul_28
- chap7_li_96Managing the contract award process (including notifying unsuccessful tenderers) and financial close.
- chap7_ul_29
- chap7_li_97Obtaining internal approvals for the health PPP project and managing other stakeholder requirements.
125chap7_p_125There must, therefore, be absolute clarity on the role and responsibilities of each member of the procuring entity’s project team.
126chap7_p_126Effective management of a procurement competition requires strict scoping of the timetable for the procurement competition, and for the procurement competition to be mapped from start to finish to allocate the necessary time and staffing resources. This is important in terms of identifying any pinch points where additional resources may be required.
127chap7_p_127An analysis must be conducted to determine the likely time commitment required from each member of the procuring entity’s project team. This will enable a procuring entity to determine whether its internal personnel (e.g. clinical, financial, technical, legal, estates, insurance/risk, etc.) should be part of the project team on a full-time basis or whether a more tailored approach using those personnel on an ad hoc basis with support from external advisors is more appropriate. In addition, thought should be given to ensuring continuity of personnel throughout the pre-procurement, procurement and contract management stages.
Duration of the Procurement Competition
128chap7_p_128The length of the procurement competition will depend on several factors, including the type of PPP being procured, the chosen procurement procedure and whether there is an urgent requirement for the procurement. Above all else, the procuring entity should not be pressured into accelerating the timescales for the procurement competition by senior officials. A typical DBFO procurement using the competitive dialogue procedure could take 18 to 24 months.
129chap7_p_129In terms of developing and applying the programme for the procurement competition, it is recommended that the following general principles be used for fixing time limits:
- chap7_ul_30
- chap7_li_98When receiving RfQ responses, pre-dialogue meeting deliverables, and tenders, procuring entities should consider the complexity of the health PPP project and the associated PPP contract.
- chap7_li_99When asked for time extensions, procuring entities should extend the time limits for the receipt of RfQ responses or tenders in the following cases:
- chap7_li_100Where additional information, although requested by the tenderer in good time, is not supplied by the procuring entity in a reasonable time before the time limit fixed for the receipt of RfQ responses or tenders.
- chap7_li_101Where significant changes are made to the tender documentation.
- chap7_ul_31
130chap7_p_130The length of the extension of time must be proportionate to the significance of the information or change. Where additional information has either not been requested promptly or its importance in preparing responsive tenders is insignificant, procuring entities do not need to extend the time limits.
Case Study: Getting the Timelines Wrong131chap7_p_131A healthcare PPP was well-structured and demonstrated strong feasibility during the feasibility study phase. However, in the subsequent procurement stage, insufficient time was allocated to assessing market appetite and effectively marketing the opportunity to potential investors. Compounding this, political pressure led the procuring authority to adopt overly ambitious timelines, including a compressed window for submission of RfQ responses. As a result, only one bidder submitted a response, forcing the procuring entity to reconsider its approach. |
Risk Allocation in Health PPP Projects
132chap7_p_132In a health PPP project, each risk should be allocated to the party best able to manage that risk. The provisions in the PPP contract should be drafted in such a way as to incentivise that party to mitigate such risk. Incentives could include performance or availability deductions, or damages and reliefs under the PPP contract.
133chap7_p_133If risk is not allocated effectively by the procuring entity in the PPP contract, unnecessary risk premiums will be levied by the private partner, meaning:
- chap7_ul_32
- chap7_li_102Less value for money for the public sector
- chap7_li_103Less market participation
- chap7_li_104Less effective competition
134chap7_p_134The approach to risk allocation varies by jurisdiction, and what may be a market norm in one country may not be in another. Additionally, different sectors have varying standards for risk allocation. The diagram below illustrates examples of typical PPP risks and health PPP risks.
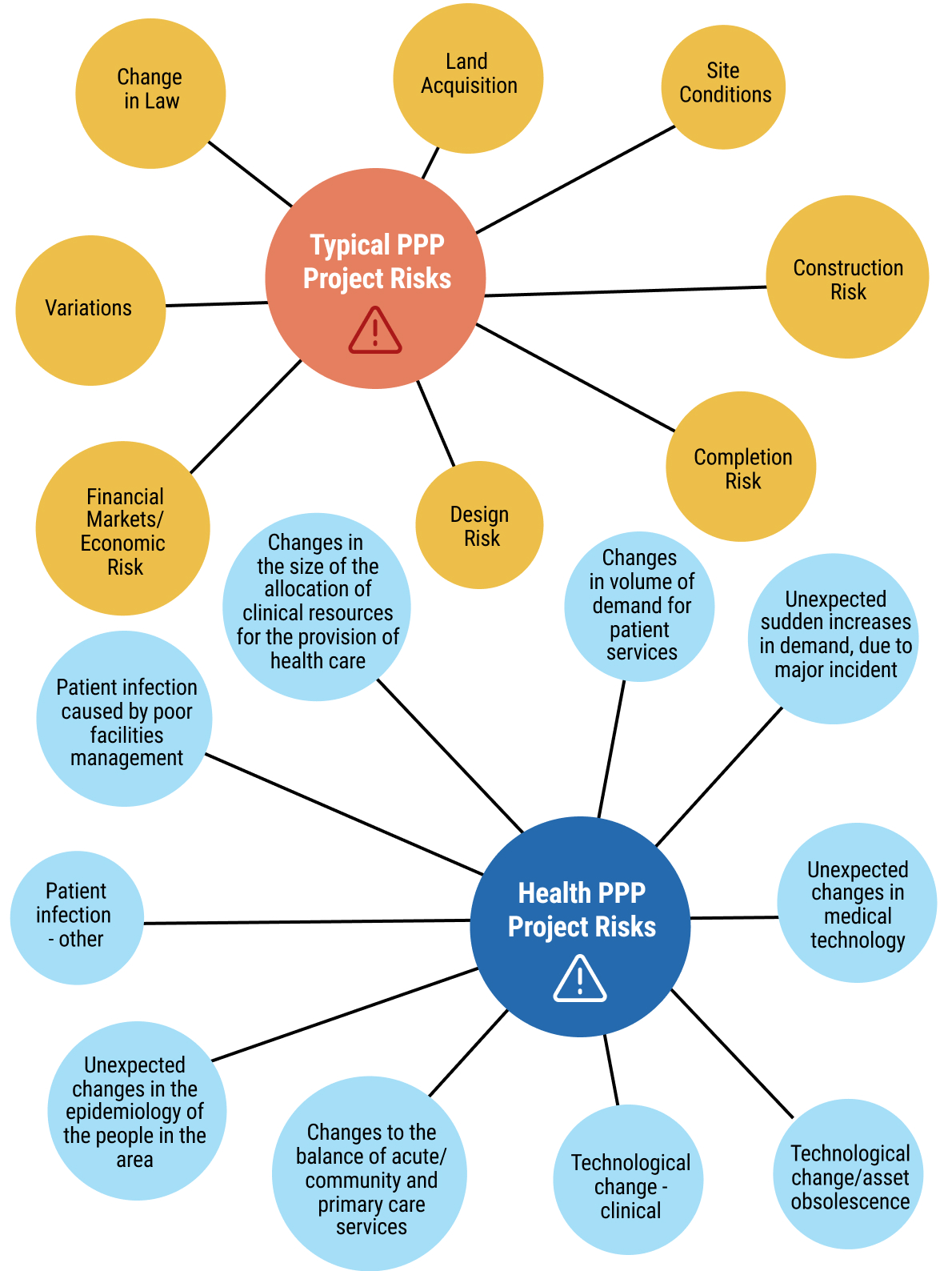 chap7_img_8
chap7_img_8
Choosing a Contractual Model for Health PPP
135chap7_p_135A range of different PPP contractual models can be used to deliver health PPP projects. Choosing the right contractual model involves considering several key factors, as illustrated in Figure 7.10 below.
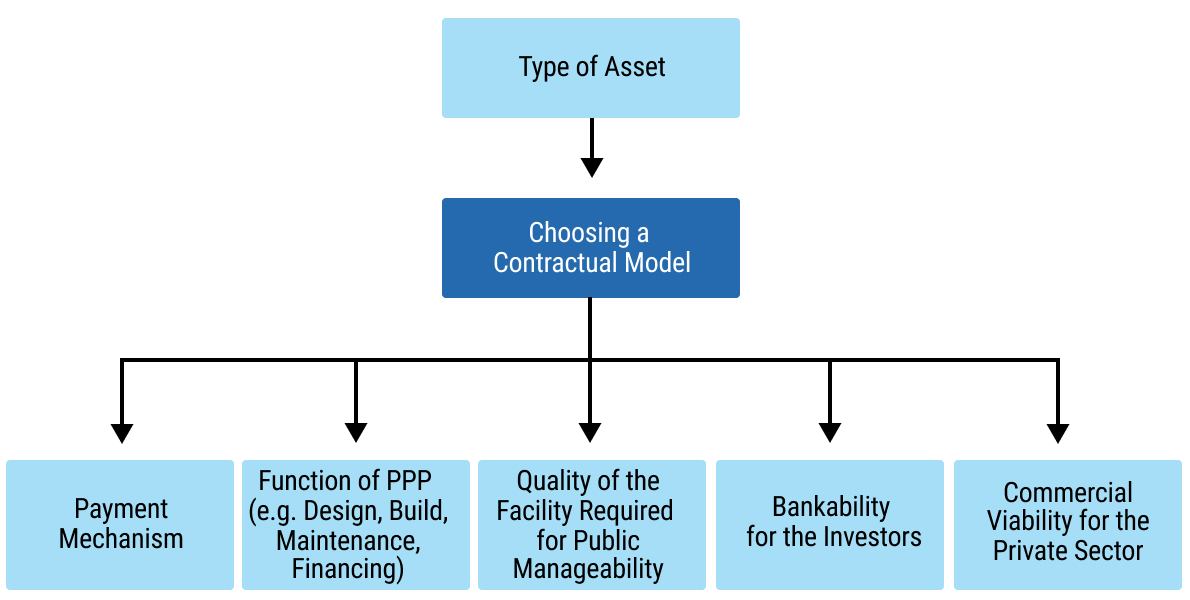 chap7_img_9
chap7_img_9
136chap7_p_136Table 7.2 below sets out a selection of the PPP contractual models which could be chosen for a health PPP.
|
137chap7_p_137PPP Contractual Model |
138chap7_p_138Type of Asset |
139chap7_p_139Overview |
140chap7_p_140Payment Source |
|
141chap7_p_141Management Contract |
142chap7_p_142Existing infrastructure |
143chap7_p_143The government retains ownership of assets and responsibility for capital expenditure. The private sector is responsible for maintenance and operation. Typically shorter in duration (3-10 years). |
144chap7_p_144Management fees are extended to the contractor |
|
145chap7_p_145Output-Based Performance Contract |
146chap7_p_146Existing infrastructure |
147chap7_p_147The private sector is provided with the freedom to meet performance requirements. |
148chap7_p_148Typically, the monthly fee from the government is based on performance indicators |
|
149chap7_p_149Build-Own-Operate- Transfer 150chap7_p_150(BOOT) |
151chap7_p_151New infrastructure |
152chap7_p_152Private sector builds, owns and maintains the asset for the duration of the contract. Handed back to the public sector upon termination or expiry of the contract. |
153chap7_p_153Government or user |
|
154chap7_p_154Build/Rehabilitate- 155chap7_p_155(BOT/ROT) |
156chap7_p_156New infrastructure |
157chap7_p_157The private sector builds or rehabilitates and maintains assets for the duration of the contract. Handed back to the public sector upon termination or expiry of the contract. |
158chap7_p_158Government or user |
|
159chap7_p_159Build-Own-Operate 160chap7_p_160(BOO) |
161chap7_p_161New infrastructure |
162chap7_p_162The private sector builds and maintains the asset for the duration of the contract. The asset is not handed back to the public sector. |
163chap7_p_163Government or user |
|
164chap7_p_164Design-Build-Finance-Operate 165chap7_p_165(DBFO) |
166chap7_p_166New infrastructure |
167chap7_p_167The private sector designs, builds, finances, operates and maintains an asset, then leases it back to the government (typically for 25-30 years). |
168chap7_p_168Government or user |
|
169chap7_p_169Build, lease, transfer 170chap7_p_170(BLT) |
171chap7_p_171New infrastructure |
172chap7_p_172The private sector builds and leases the asset back to the government. Handed back to the public sector upon termination or expiry of the contract. |
173chap7_p_173Government 174chap7_p_174or user |
|
175chap7_p_175Concession |
176chap7_p_176New or existing infrastructure |
177chap7_p_177Varies depending on the jurisdiction, but typically, a grant by a government of the right to provide a service or use an asset. |
178chap7_p_178User |
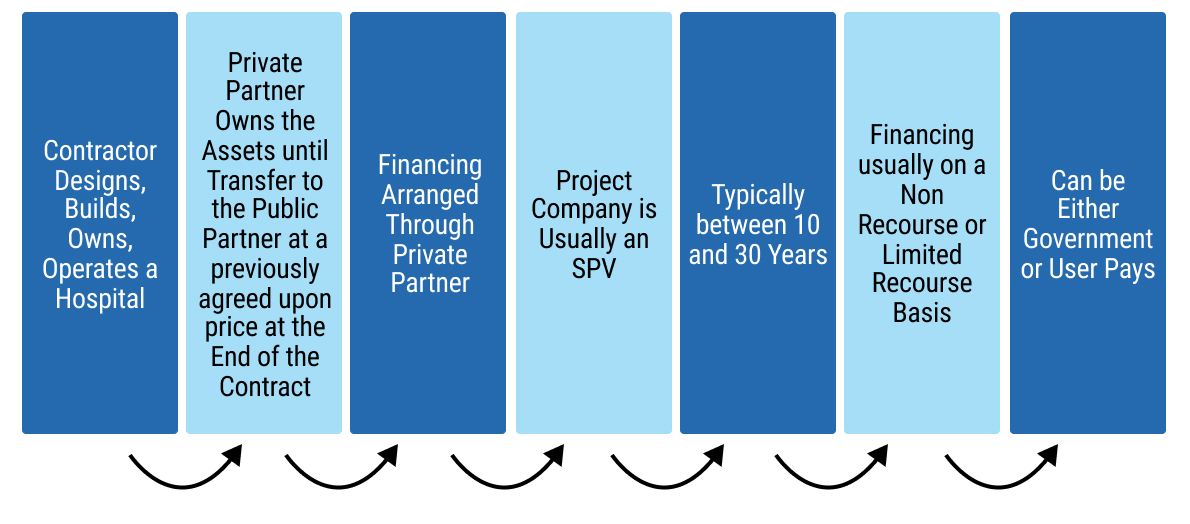 chap7_img_10
chap7_img_10
179chap7_p_179To further assist in selecting the right PPP contractual model for a health PPP project, the appraisal criteria and considerations outlined in Table 7.3 below should be applied.
|
180chap7_p_180Appraisal Criteria |
181chap7_p_181Considerations |
|
182chap7_p_182Accessibility of Public Medical Services |
183chap7_p_183The potential for the PPP model to provide health care and services to patients (including patients who may not be insured or able to pay for medical care). |
|
184chap7_p_184Quality of the Project |
185chap7_p_185The potential for the PPP model to deliver a good quality project, resulting in a positive experience for patients and staff. |
|
186chap7_p_186Manageability of the Project |
187chap7_p_187The potential for the PPP model to be within the capability of the procuring entity to effectively administer, including (i) management and delivery of the procuring entity’s responsibilities in the PPP contract, and (ii) ensuring that the private partner is effectively managed in accordance with the terms of the PPP contract. |
|
188chap7_p_188Potential for Better Value-for-Money |
189chap7_p_189The potential for the PPP model to offer a good combination of price and quality risk in the delivery and operation of the PPP project. |
|
190chap7_p_190Potential for Lifecycle Optimisation |
191chap7_p_191The potential under the PPP model is that the design and construction of the PPP project can be optimised to present the best value over the lifetime of the PPP project. |
|
192chap7_p_192Leveraging Key Private Sector Capabilities |
193chap7_p_193The extent to which the private sector will be capable of being involved in, and performing its required role under, the PPP model. |
|
194chap7_p_194Commercial Viability of the PPP Project for the Private Sector |
195chap7_p_195Will there be sufficient commercial potential and interest for private operators (and investors) in the PPP model? |
|
196chap7_p_196Bankability for Investors |
197chap7_p_197The extent to which the PPP model will allow for the provision of sufficient (debt) financing. |
|
198chap7_p_198Potential for Competitive Procurement |
199chap7_p_199Whether the PPP model will allow for sufficient competition in the procurement. |
The Health PPP Project Agreement
200chap7_p_200The PPP contract, also known as the project agreement, is the key contract that the procuring entity is required to enter into with the private partner, in connection with, for example, the DBFO of the health PPP project being procured. Figure 7.12 below illustrates the location of the project agreement within a DBFO contractual model, as well as the key contracting parties and other contracts that form part of the DBFO contractual model.
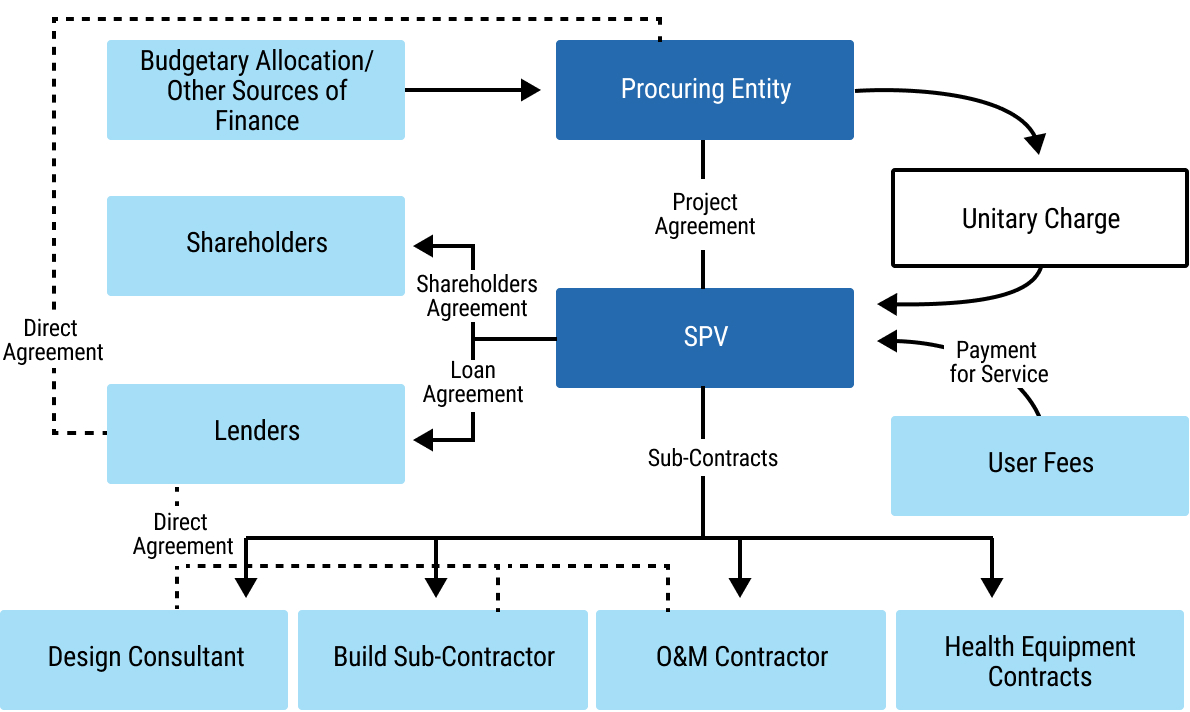 chap7_img_11
chap7_img_11
201chap7_p_201The project agreement should be developed by the procuring entity prior to the commencement of the procurement competition and will then be the subject of dialogue or negotiation (in the context of a competitive dialogue or negotiated procurement procedure) between the procuring entity and tenderers.
202chap7_p_202The development of the project agreement should reflect the outcome of the risk identification and allocation process, which should have been undertaken with respect to the health PPP project. In addition to the normal matters which are considered in the development of a project agreement (e.g. grounds for termination and compensation on termination, dispute resolution, force majeure and land issues, amongst many others), key issues for the development of a project agreement for a health PPP include consideration of:
- chap7_ul_33
- chap7_li_105Maintenance. Does the scope of the project agreement include soft facilities management (soft FM) and hard facilities management (hard FM) or just hard FM? Hard FM relates to the physical aspects of buildings. This means that any service carried out on a bodily structure falls under hard FM. Often, hard FM services are required by law to ensure that facilities are safe for staff, patients and any visitors. Hard FM services include: fire safety services, gas maintenance, plumbing, heating, ventilation, air conditioning, building maintenance, electrical and lighting maintenance and accessibility maintenance. Soft FM relates to services which ensure buildings maintain a secure and pleasant environment. Soft FM services include waste management, cleaning services, grounds maintenance and landscaping, security services, catering, pest control and janitorial services.
- chap7_li_106Technological change. Suppose health equipment is part of the scope for the PPP contract. In that case, the contract must include mechanisms to adapt to rapid technological and medical advancements, such as new equipment or treatment protocols.
- chap7_li_107Epidemic/pandemic response. Specific clauses defining roles, responsibilities and financial implications in the event of a public health crisis (e.g. pandemic response) should be included, ensuring seamless integration into national emergency plans.
- chap7_li_108Interoperability. When the provision of information technology (IT) systems is included in the scope of the PPP contract, consideration should be given to ensuring that the private partner’s IT systems are compatible and interoperable with existing national or regional health information systems, thereby facilitating continuity of care and public health monitoring.
- chap7_li_109Data sharing and ownership. Clearly, healthcare generates sensitive patient data. If the private partner will have access to patient data, there should be explicit clauses regarding data ownership, privacy, security and protocols for sharing data with public health authorities.
- chap7_li_110Output-oriented specifications. If appropriate, the scope of the PPP contract should move beyond merely specifying infrastructure (e.g. number of beds) to defining the desired health outcomes (e.g. healthcare-associated infection rates, readmission rates, wait times).
- chap7_li_111Patient safety and risk management. Clear protocols for identifying, managing and reporting clinical risks and incidents should be included in the PPP contract.
- chap7_li_112Clinical effectiveness and audit. Mandating regular clinical audits against national and local standards to ensure best practices are followed should be included in the PPP contract.
- chap7_li_113Stakeholder engagement. Provisions in the PPP contract should outline communication and engagement processes between the public partner, private partner, healthcare professionals and patient representatives to foster trust and proactively manage issues.
Management of the PPP Contract
203chap7_p_203The procuring entity is responsible for ensuring that a PPP contract is administered correctly and enforced in accordance with its terms and conditions. For this purpose, it is recommended that the procuring entity:
- chap7_ol_1
- chap7_li_114Establishes a contract management team which will oversee the administration of the PPP contract. Ideally, this team should include personnel who have been involved in the procurement of the health PPP project.
- chap7_li_115Provides the necessary resources, including human resources, to its contract management team to enable effective contract administration,
- chap7_li_116Appoints where required, technical, financial and legal experts as members of the procuring entity’s contract management team to assist with any aspect of the administration or enforcement of the PPP contract, which may include:
- chap7_li_117In respect of the legal expert, interpretation of the terms and conditions of the PPP contract, variations of the PPP contract, termination of the PPP contract and disputes in connection with the PPP contract.
- chap7_li_118In respect of the financial expert, operation of the payment mechanism, audit and accounting regarding the PPP contract, variations of the PPP contract and the operation of performance guarantees.
- chap7_li_119In respect of the technical expert, design and construction, completion and commissioning, defects rectification, operation and maintenance, variations of the PPP contract and handback and transfer issues.
- chap7_ul_34
204chap7_p_204The procuring entity, supported by its contract management team, should establish procedures for the administration of each PPP contract, and these should include:
- chap7_ol_2
- chap7_li_120Managing governance of the PPP contract (which should include a process for the recording and communication of the appropriate decision-making authorities in respect of the PPP contract).
- chap7_li_121Communicating and liaising with the private partner (which should include the preparation of a comprehensive communications plan) and any independent engineer or third party who has been appointed pursuant to the PPP contract.
- chap7_li_122Monitoring, evaluating and regulating the performance by the private partner of the PPP contract and the implementation of the health PPP project by the private partner (which should include the preparation of a comprehensive contract management plan).
- chap7_li_123Measuring outputs related to the performance of the private partner in terms of the PPP contract, including the involvement in such measurement by any independent engineer or third party who has been appointed pursuant to the PPP contract.
- chap7_li_124Receiving, reviewing and addressing issues arising from reports submitted by the private partner to the procuring entity pursuant to the PPP contract.
- chap7_li_125The provision of reports by the private partner to the procuring entity in respect of the health PPP project and its progress, including but not limited to achievements, challenges, obstacles and outstanding issues.
- chap7_li_126Ensuring that all rectification measures are undertaken by the private partner on a timely basis and performance regimes are strictly and timeously enforced in accordance with the PPP contract.
- chap7_li_127Management responsibilities including managing stakeholder engagement, managing any variation, termination or dispute, managing transfer or handback of the health PPP project and managing accounting, audit and other compliance and regulatory matters.
205chap7_p_205Where relevant in the context of the type of health PPP project, it is recommended that the procuring entity, supported by its contract management team, establishes a procedure for the transfer or handback of the asset comprised in the PPP project on the occurrence of the date of expiry of the PPP contract. Such a procedure should ensure that the asset is handed back or transferred to the procuring entity in a condition which is in accordance with the terms of the PPP contract, with the required documentation for the procuring entity or another private partner to manage and operate the asset. Such a procedure may also include:
- chap7_ul_35
- chap7_li_128Joint inspection by the procuring entity and the private partner to assess the condition of the asset before transfer or handback.
- chap7_li_129Pursuant to such joint inspection, identification of any remedial measures which need to be taken by the private partner (at the private partner’s cost) before the asset is transferred or handed back to the procuring entity.
206chap7_p_206The procuring entity should also give consideration regarding its reporting obligations under law (or procedure) to other public entities (e.g. PPP unit, audit office). Reports could include details with respect to:
- chap7_ol_3
- chap7_li_130The relevant project and its progress.
- chap7_li_131Any achievements of the procuring entity in respect of the PPP project.
- chap7_li_132Any challenges or obstacles which the procuring entity has encountered in respect of the PPP project, and how the procuring entity dealt with those challenges or obstacles.
- chap7_li_133Any outstanding issues in respect of the PPP contract and how the procuring entity plans to deal with those outstanding issues.
- chap7_li_134The performance of the private partner as measured against the requirements of the PPP contract.
- chap7_li_135Any variations or disputes under the PPP contract.
- chap7_li_136Any preparations for transfer or handback of the PPP project.
- chap7_li_137Any local development opportunities and any community involvement (e.g. support to local businesses, technology or skills transfer, job creation).
Case Study: Failure of the Government to Deliver its Obligations Under the PPP Contract207chap7_p_207A government procured specialised medical equipment under a PPP arrangement for public hospitals across the country. The installation of the equipment requires prerequisite works at the beneficiary facilities, including an adequate water supply, three-phase power and other necessary infrastructure upgrades to meet the specified technical standards. 208chap7_p_208However, several facilities were not adequately equipped to meet these requirements and lacked the necessary funding to undertake the preparatory works. Consequently, the contractors were unable to install the equipment as scheduled, resulting in significant portions of the equipment remaining in storage for extended periods while the facilities sought to upgrade their infrastructure. 209chap7_p_209During this period, the contractors continued to be entitled to availability payments, as the delay in equipment installation was attributable to the public entities. As a result, the public sector incurred financial obligations without the corresponding service benefits and the intended health outcomes and value-for-money objectives of the PPP. 210chap7_p_210A key lesson from this experience is that procuring entities must be fully prepared to fulfil their obligations under any PPP contract. In this case, a robust contract management team could also have helped anticipate potential performance issues, ensuring that the PPP delivered its full intended value. |
Chapter 8: Credit Enhancement
Key Takeaways
|
1chap8_p_1This chapter outlines the various credit enhancement mechanisms that may be used in the three instruments described in this User Guide: sustainable finance instruments, debt-for-health swaps, and health public-private partnerships (PPPs) and explains how these mechanisms strengthen the bankability and overall feasibility of health financing transactions.
What is Credit Enhancement, and Why is it Important?
2chap8_p_2Broadly, credit enhancement can be defined as a financial mechanism designed to improve the creditworthiness of a borrower or a specific transaction and includes, among others, guarantees and guarantee-like instruments, insurance, or a combination thereof. As their primary purpose is to share and/or mitigate risk, thereby improving financing terms (including new financing sources, larger volumes, longer tenors, grace periods, and more favourable pricing), these mechanisms play a key role in unlocking financing for governments.
Credit Enhancement for Sustainable Finance Instruments and Debt Conversions
3chap8_p_3In the sovereign finance context, credit enhancement may be provided by multilateral development banks (MDBs), DFIs, ECAs, or private insurers. Sustainable finance instruments can benefit from various forms of credit enhancement, including (i) partial credit guarantees, (ii) political risk insurance, and (iii) collateralisation.
In PPPs exposed to political risks, such as the risk of non-payment by a government or a government-owned entity, or breach of contracts, MDBs also offer partial risk guarantees (PRGs) on government obligations to encourage lenders and investors to participate. In each case, the financial structure and the choice of credit enhancement mechanism need to be tailored to the specific context. In the case of sustainability-linked loans (SLL) and debt swaps, the credit enhancement mechanism needs to reflect the country’s financial situation, implementation capacity, and policy objectives. For health PPPs, credit enhancement mechanisms are informed by the project type and model. Note that there is a growing trend to combine multiple credit enhancement mechanisms to maximise coverage and further reduce the overall cost of financing operations.
4chap8_p_4The following details the most standard credit enhancement tools used in sovereign sustainable finance transactions:
1. Partial Credit Guarantees
Description and Rationale
5chap8_p_5PCGs provide an irrevocable and unconditional commitment from a guarantor to cover a specified portion of scheduled debt service in the event of default by the borrower or issuer. They can be structured to cover any category of risk that could trigger a payment default, including credit or project-related risks. This type of credit enhancement enables the instrument to benefit from the guarantor’s higher credit rating, resulting in more favourable financing terms, such as lower interest rates, longer maturities, and larger financing volumes. In Africa, PCGs for sovereign or sovereign-guaranteed borrowers could be offered by multilateral and regional development banks such as the African Development Bank (AfDB), the World Bank Group through its new guarantees platform, the European Investment Bank (EIB), Asian Infrastructure Investment Bank (AIIB), the African Export-Import Bank, Africa Finance Corporation and others. Other development finance institutions, such as GuarantCo, focus their PCGs on supporting private sector borrowers, including project companies in PPPs and sub-national entities.
6chap8_p_6Within the broad category of PCGs, there are investment guarantees, which support a specific project, and policy-based guarantees, which are linked to the implementation of agreed policy reforms by a sovereign. PCGs can also take the form of portfolio guarantees when they cover a portfolio of transactions (for instance, a PCG can cover a portfolio of loans to health institutions to be constituted by a lender). Another form of PCG is the transaction guarantee offered by the AfDB to support trade transactions specifically (such as the import of medical equipment).
Rationale
7chap8_p_7Under PCGs, and in the context of a loan or bond, the lenders or bondholders benefit from a guarantee agreement with one or more guarantors, who undertake to cover a defined portion of scheduled debt service payments in the event of default by the borrower. The borrower, in turn, typically enters into a counter-indemnity agreement with the guarantor, under which it commits to reimburse the guarantor for any amounts paid under the guarantee.
8chap8_p_8To increase the PCG amount they can provide, MDBs can utilise a guarantor-of-record structure, where risk participants, including co-guarantors and credit insurers, can participate in the exposure while the MDB fronts the guarantee.
9chap8_p_9Figure 8.1 represents the financial structure of a sustainable loan with a PCG. Refer to Chapter 4: Health Finance and Key Performance Indicators for a detailed discussion of sustainable finance instruments.
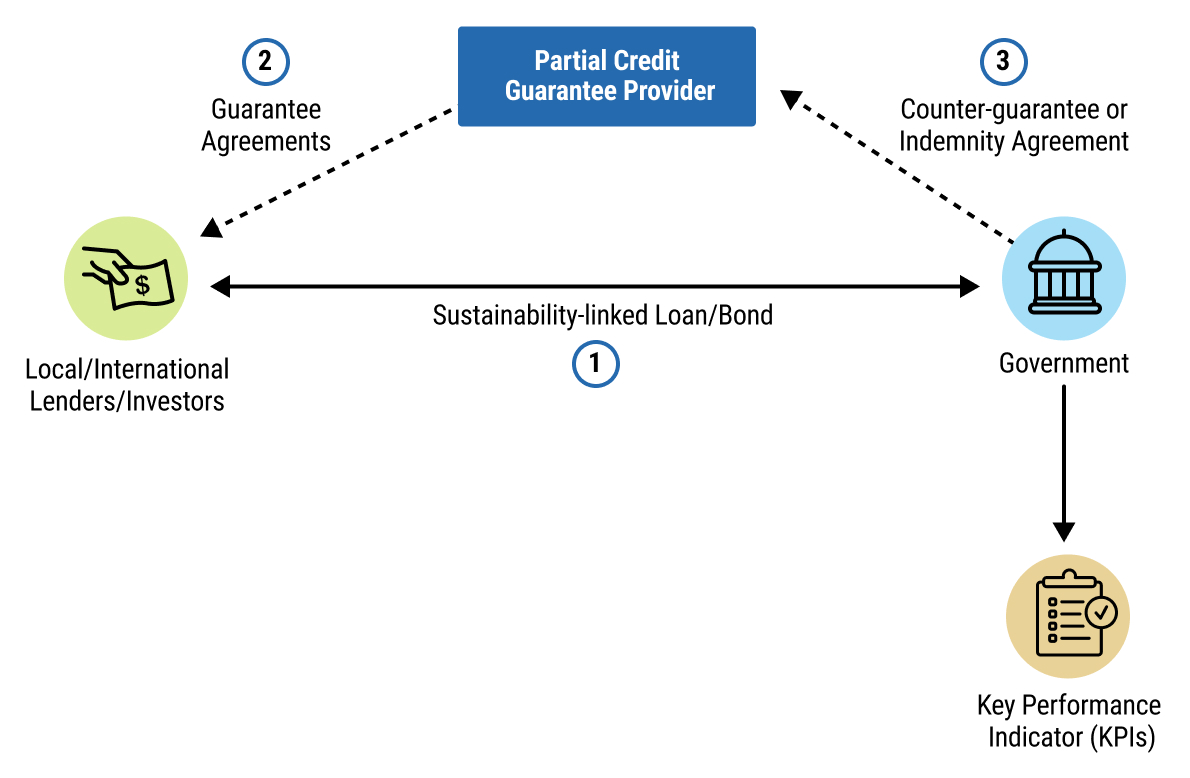 chap8_img_0
chap8_img_0
10chap8_p_10In the context of a commercial debt-for-health swap (also known as debt conversion), credit enhancement is used to de-risk the new-money transaction and attract private investors by partially or fully guaranteeing payments under the new debt instrument. As such, the credit enhancement will cover only the debt being issued to finance the buyback. The government will utilise the proceeds from the newly issued, credit-enhanced debt to retire outstanding, and/or more expensive discounted debt, thereby generating fiscal savings that will be used to fund agreed-upon health sector investments or programmes. Refer to Chapter 5: Sustainable Finance Instruments for a detailed discussion of debt conversions.
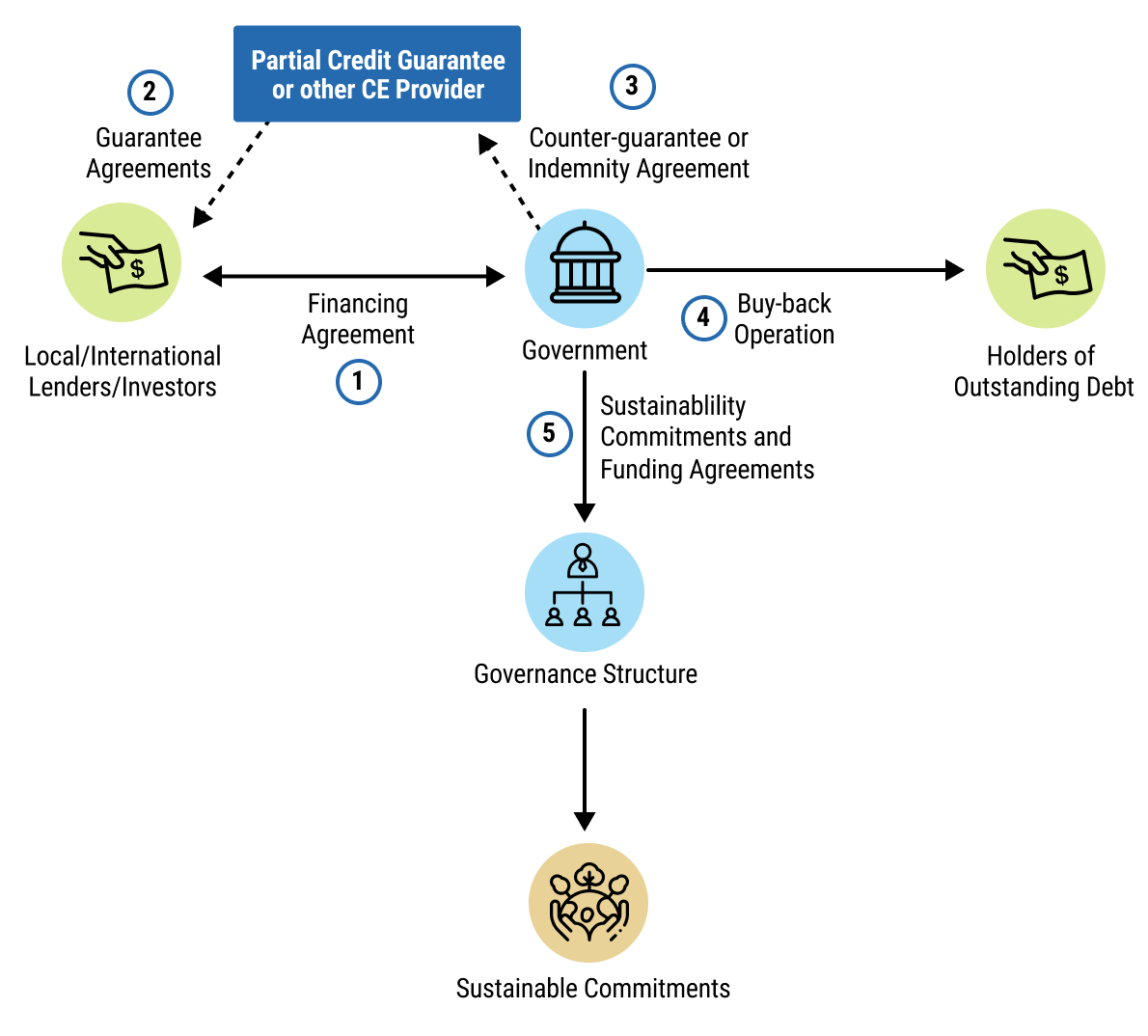 chap8_img_1
chap8_img_111chap8_p_11Notably, in recent debt conversions, PCGs have often been combined with PRI, other public or private co-guarantees, or private credit insurance instruments to mobilise additional private capital and enhance the scale and developmental impact of the transactions.
12chap8_p_12PCGs can support governments, government-owned entities and private sector entities in their debt mobilisation efforts to fund healthcare projects.
2. Political Risk Insurance
Description and Rationale
13chap8_p_13PRI can protect investors against non-commercial risks such as expropriation, currency inconvertibility, political violence, breach of contract by a government or state-owned entity, or sudden regulatory changes. For example, the U.S. DFC provides PRI that explicitly covers losses resulting from the borrowing country’s non-payment of a final and binding arbitral award and from denial of access to justice. In Africa, PRIs are provided by multilateral institutions such as the World Bank Group’s MIGA, DFIs such as African Trade and Investment Development Insurance, and private insurers.
14chap8_p_14Unlike PCGs, which are generally unconditional, PRI payouts are contingent on predefined political events that must be verified. Because the payout may be linked to the conclusion of a lengthy process, such as international arbitration, PRI may be combined with guarantees or collateralisation to ensure continuity of payments. In contrast, the arbitration is being pursued to maintain investor confidence. Providers of PRI may not require counter-guarantees but will seek to have subrogation rights (I.e. the right of the insurer to step into the shoes of the insured party and to recover from any third party responsible for the loss) - I.e. the credit enhancement provider steps into the investor’s shoes in respect of the right to recover amounts covered by the PRI.
Rationale
15chap8_p_15A common practice in debt conversions has been to establish an SPV to issue bonds to investors or enter into a loan agreement with lenders. The SPV will then on-lend the proceeds through a new loan agreement with the government. This new lending arrangement may be credit-enhanced by a PRI that covers the loan principal amount and will often be combined with a liquidity guarantee, ensuring that interest payments will still be made to investors prior to the policy paying out.
For example, when the policy covers failure to pay an arbitral award, the liquidity guarantee would cover any interest payments incurred during the arbitration proceedings. This liquidity guarantee could be established as a PCG or as a collateralisation mechanism, where specific assets or cash are set aside as security.
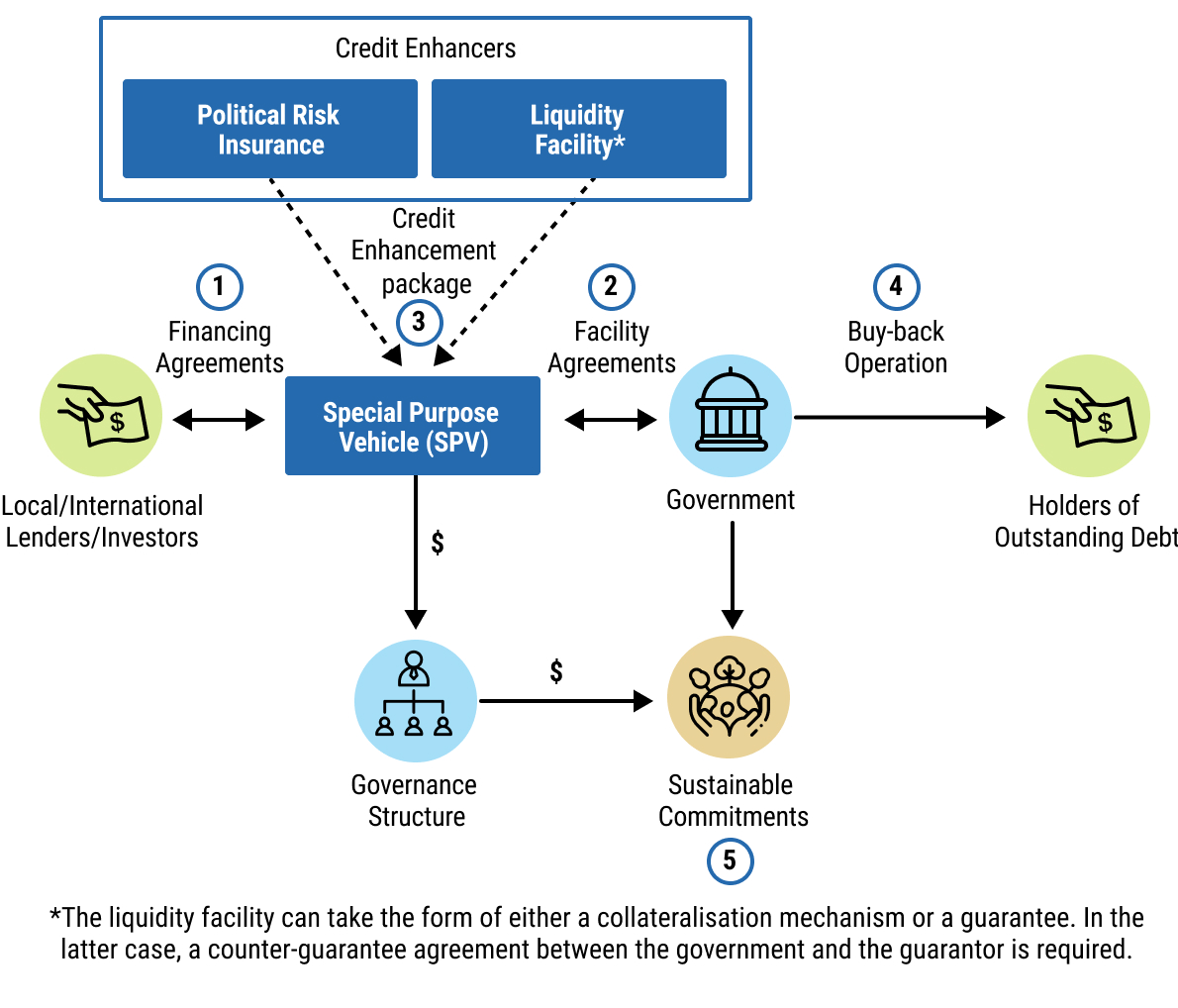 chap8_img_2
chap8_img_2
3. Collateralisation
Definition and Rationale
16chap8_p_16A collateralisation mechanism is a way to set aside certain of the borrower’s assets or revenue stream that can be used to repay lenders if the borrower is unable to meet its repayment obligations. Government assets that generate stable or predictable income (e.g. export proceeds, tax revenues, or project-related cash flows) or the income itself can serve as collateral. This provides additional comfort to lenders and typically improves borrowing terms.
17chap8_p_17These mechanisms can be employed to back a guarantee for a portion of transactions or ensure debt service payments in the event of a default. Collateralisation of a guarantee gives creditors rights over a guarantor’s or borrower’s asset(s) or revenue stream that, in the case of default, could allow the creditor to secure repayment of the debt.
Rationale
18chap8_p_18Where collateralisation is used, the borrower and its creditors will enter into agreements that define the rights and obligations related to the pledged assets, including enforcement rights, such as a collateral or security agreement.
19chap8_p_19From a legal standpoint, the borrower must avoid breaching any negative pledges to which they may be bound under the underlying contractual agreement (such as those imposed by the World Bank or other relevant entities providing credit enhancement). From a fiscal standpoint, collateralised loans represent contingent liabilities that need to be disclosed and accounted for, with a potential impact on debt sustainability. Revenue collateralisation may limit budget flexibility if the collateral is called upon.
4. Partial Risk Guarantees (PRGs)
Definition and Rationale
20chap8_p_20PRGs cover a private project in relation to relevant government or government-owned entity undertakings and/or politically-related risks vis-à-vis the project and not genuine commercial risks. Government undertakings towards a private project can be of a financial or non-financial nature, and these undertakings shall be clearly defined in contracts between the government and the private project or its sponsor. A PRG can attract investments (debt and/or equity financing) in project finance transactions where a project’s success depends as much on government undertakings as on private commercial acumen. In public-private partnerships, PRGs can assure private partners and commercial financiers that the government will fulfil its obligations to the partnership.
Rationale
21chap8_p_21Risk coverage under the PRG can be requested for protection against political risks such as non-payment, breach of contract, currency inconvertibility or confiscation/expropriation. These are mainly the same as those covered under PRIs. However, unlike PRIs, PRGs do not require an arbitration process. Following non-payment by the government or a government-owned entity, the guarantee can be called immediately upon expiration of any agreed-upon waiting period.
22chap8_p_22Similar to PCGs, PRGs generally require a sovereign counter-indemnity, where the country commits to repay any amount paid by the guarantor under the guarantee. However, some MDBs, such as the AfDB, can provide both PCGs and PRGs without sovereign counter-indemnity, provided the guarantee is commercially priced.
23chap8_p_23The PRG can support a project mainly through two types of structures: (i) PRG with a deemed loan provided to the beneficiary for protection against termination risk and (ii) PRG with a standby letter of credit for protection against temporary liquidity shortfalls from the government or a government-owned entity.
chap8_img_3Combining Credit Enhancement Sources
24chap8_p_24Credit enhancement instruments provided by MDBs and DFIs may also be combined with private sector credit enhancement, thereby strengthening the credit profile of the underlying transaction and further improving finance terms.
25chap8_p_25A notable example of blended credit enhancement is Côte d’Ivoire’s inaugural SLL issued in 2025, which combined two distinct MDB products: a policy-based guarantee from the World Bank Group’s International Bank for Reconstruction and Development (IBRD) and a non-honouring of sovereign financial obligations guarantee from MIGA. This innovative structure provided AAA-rated coverage for 95% of the loan, significantly reducing the all-in cost of borrowing and enhancing investor confidence.
26chap8_p_26The following outlines how private sector instruments can complement MDB and DFI credit enhancement support.
Private Sector Insurance
27chap8_p_27Private insurers increasingly participate in sovereign transactions by covering a portion of the payment risk related to sovereign or sub-sovereign obligations through credit insurance policies, reinsurance arrangements, or co-insurance structures, especially when MDBs or DFIs provide anchoring guarantees and first-loss protection. This is beneficial to all parties involved as it allows lenders and development institutions to reduce risk exposure and free balance sheet capacity, enables insurers to diversify into underrepresented markets, and signals investor confidence, which ultimately improves pricing.
Private Investors as Co-guarantors
28chap8_p_28High-net-worth investors are increasingly well-positioned to share sovereign risk alongside traditional guarantors. This approach was demonstrated in the 2024 Bahamas debt-for-nature swap, where Builders Vision provided a USD 70 million co-guarantee alongside the Inter-American Development Bank (IDB) and AXA XL, an insurance and reinsurance company. This is the first example of a private investor providing credit enhancement for a sovereign debt swap transaction. Recent initiatives include the Private Credit Enhancement Facility (PCEF) by Enosis Capital, a pooled credit enhancement facility for family offices and foundations, aiming to scale the successful example of impact investor participation in sustainability-linked financing (SLFs). The PCEF is designed as a USD 1 billion facility focused on emerging market and developing economies (EMDEs), offering guarantees to share risk alongside MDB-backed transactions. Funders, including family offices, foundations, and endowments, have the option to pledge a portion of their fixed-income portfolios as collateral, retaining ownership unless a default occurs. The structure enables funders to maintain the underlying asset yield and earn a deployment premium while amplifying the impact on nature and climate outcomes.
Credit Rating Implications
29chap8_p_29Credit ratings play a critical role in determining the effectiveness and market impact of credit enhancement mechanisms. Enhancements provided by highly rated entities, such as MDBs or DFIs, can materially improve the perceived credit quality of sovereign or sub-sovereign borrowers by blending their ratings with those of the credit enhancer. It is essential to acknowledge that particular challenges exist in this regard, including uncertainty regarding how credit rating agencies and regulatory frameworks evaluate credit-enhanced instruments, particularly with respect to partial coverage and the treatment of first-loss coverage from the perspective of the credit enhancement provider. Nonetheless, it remains that well-structured credit enhancement mechanisms can improve investor confidence and improve financing terms.
Credit Enhancement for Health PPPs
30chap8_p_30Credit enhancement plays a crucial role in mitigating risk in health PPP transactions. Similar to the above, credit enhancement mechanisms in the PPP context help improve creditworthiness, which in turn enhances financing terms, thereby allowing governments to attract private investment at lower costs. As will be discussed in more detail in this section, credit enhancement can either come from external sources, such as multilateral, regional or national institutions, or from the government itself, through contractual commitments or government support mechanisms. The appropriate form of credit enhancement will depend, among other factors, on the project’s risk profile and the degree of comfort required by lenders and investors.
External Credit Enhancement
31chap8_p_31External credit enhancement in PPPs involves instruments provided by third-party institutions, such as MDBs, ECAs, DFIs and insurers. These entities use their stronger credit rating to share or absorb project risks that the government or investors would otherwise bear.
32chap8_p_32Standard external credit enhancement mechanisms include PRGs and PRI as described above.
Government-provided Credit Enhancement
33chap8_p_33Government-provided credit enhancement involves contractual commitments or financial arrangements made directly by the government to assure the private partner under the PPP contract and lenders. These instruments vary in the level of fiscal exposure they create, ranging from unconditional guarantees (the highest commitment level) to letters of support (lower commitment level). This subsection will review the two most prominent government-provided credit enhancement mechanisms found in the health PPP context.
1. Sovereign guarantees
Description and rationale
34chap8_p_34Sovereign guarantees may take various forms and can be provided in favour of multiple participants in a health PPP project (for example, to the private partner under the PPP contract or to lenders).
35chap8_p_35Sovereign guarantees typically cover the risk of non-payment and/or the risk of non-performance of other obligations. Of course, when considering the role of a government as a guarantor, it is more likely that the guarantee covers non-payment risks, as it may not have the means to fulfil (or procure the fulfilment of) other types of obligations.
36chap8_p_36It should be noted that, in some jurisdictions, providing a sovereign guarantee is not permitted under law. In such cases, alternative methods for giving comfort to the private partner under the PPP contract or lenders should be considered.
Rationale
37chap8_p_37Non-payment guarantees may relate directly to loans (to protect against debt service defaults, and which will be provided in favour of lenders) or to other payment obligations (which are not loan-related, and which will be provided in favour of the relevant private partner under the PPP contract). An example of the latter would be a guarantee regarding an off-taker’s payment obligations, or a guarantee that the revenue for a project will at least meet a certain minimum level.
38chap8_p_38A government may offer a sovereign guarantee in respect of a PPP project to enhance the project’s financial viability and bankability for lenders. The presence of a sovereign guarantee can also help to attract private sector investment, in particular foreign investment, as the private partner under the PPP contract is assured that the project has the backing of the government, which helps to mitigate the perceived risks the private sector would otherwise potentially not take on.
39chap8_p_39However, given that sovereign guarantees create potential liabilities for governments, the necessity of granting a sovereign guarantee must be reviewed on a case-by-case basis to assess whether issuing a sovereign guarantee is necessary and appropriate. Sovereign guarantees should not be provided as a matter of routine for all projects, and governments should carefully analyse the level of risk they are taking on, on a project-specific basis.
40chap8_p_40The terms of any sovereign guarantee need to be carefully considered, and the government’s exposure to liability under the terms of the sovereign guarantee should be limited as far as possible. Additionally, when providing a sovereign guarantee, a government must consider the treatment of this guarantee for accounting purposes, as it may be recorded as a contingent liability on its balance sheet.
2. Letters of Comfort
Description
41chap8_p_41The host country provides a letter of comfort in which it promises to facilitate a project through, for example, facilitating certain approvals required for project implementation. Such a letter may be provided in place of a government guarantee where the guarantee would require parliamentary or constitutional approval or where granting a guarantee would negatively impact the sovereign’s debt sustainability levels.
Rationale
42chap8_p_42A letter of comfort does not establish a legally binding obligation; rather, it reflects the sovereign’s intent to support the project. As such, this type of credit enhancement provides a lower level of protection for the lender or investor.
43chap8_p_43Where applicable, the letter should address the lender’s areas of concern regarding the PPP project.
44chap8_p_44In some cases, a government letter may be enhanced to include firm undertakings, transforming the letter into a legally binding obligation.
3. Letters of Support
45chap8_p_45A letter of support is a government instrument issued to a private party, providing assurances that the government will cover certain political, legal, and regulatory risks. The scope of coverage typically varies from country to country. It is, however, not a sovereign guarantee.
4. Other Types of support
46chap8_p_46Governments can also offer other forms of support, such as providing grants or subsidies for a PPP project, tax breaks, or customs exemptions. Often, a combination of measures is taken.
47chap8_p_47In addition, contract terms (e.g. indemnities and compensation on termination) can also be used to provide relief in the event of specific risks, as opposed to covering those risks through a sovereign guarantee. Please note that contractual indemnities from governments attract the same contingent liability issues as sovereign guarantees. For detailed description of contingent liabilities, please see Understanding Sovereign Debt: Options and Opportunities for Africa
5. General Considerations
48chap8_p_48It is essential when considering credit enhancement to understand the expenses the credit enhancement provider expects the sovereign to cover, the premium payment to be paid, and the timing of such payments. Understanding the legal basis upon which such credit enhancement is to be provided will also be important, especially any recovery routes that the credit enhancement provider will require (e.g. counter-guarantees/indemnities, subrogation rights, transfers/assignments of commitments, etc.). Credit enhancement providers will also have specific participation conditions, and understanding these early on in the transaction structuring process will be helpful. They will also have their own internal approval processes for participation in any transaction, and these should be factored into the project timeline.
Chapter 9: Recommendations
Call to Action
1chap9_p_1At a time when drastic aid cuts and debt challenges are significantly impacting health spending in Africa, there is a need to consider sustainable financing alternatives to support public health initiatives and improve public health provisioning. Health is not only essential for individual well-being but also for economic growth and societal resilience. Investing in strong health systems remains a top priority for both citizens and governments in Africa. As some African countries pursue short-term responses to health aid cuts, there is a need to think of long-term financial solutions to support health investments and programmes.
2chap9_p_2Concurrently, there is an excellent opportunity to leverage innovative financial tools that have been broadly deployed outside of the health sector. These tools have evident financial benefits, including reduced costs of finance and the delivery of critical development outcomes. This is even more true when catalysing the participation of development finance institutions (DFIs) and donors, who are highly interested in supporting global health. To capitalise on these opportunities, both the Ministry of Finance (MoF) and Ministry of Health (MoH) must collaborate to achieve better financial and health outcomes for their country.
Recommendations for Ministries of Health
- chap9_ol_0
- chap9_li_0
3chap9_p_3Advocate for fair and realistic allocations to health.
4chap9_p_4MoHs will need to regularly make the case for debt-raising resources to be allocated to health financing and to ensure that allocated budgets and resources are sufficient to deliver the agreed outcomes or ambitions. This requires balancing ambition with realism - setting achievable targets while using the visibility of debt-linked commitments to advocate for greater budget allocations over time. It also requires annual advocacy during the budget cycle to ensure relevant activities continue to be prioritised.
- chap9_li_1
5chap9_p_5Take a long-term, strategic view in financing health priorities.
6chap9_p_6To engage effectively with MoFs on budget allocation, debt instruments and public-private partnership (PPP) arrangements, MoHs must first define where additional resources are most needed and how these align with national development goals and national health plans. This means articulating clear long-term priorities and identifying specific, well-scoped projects or programmes that could be financed through mechanisms such as PPPs, debt swaps or sustainable finance instruments. A forward-looking investment plan gives MoFs confidence that health proposals are not short-term or ad hoc, but part of a coherent national strategy. In the case of PPPs for hospitals or health facilities, this includes developing a health master plan, as described in Chapter 6: Debt-for-Health Swaps, to anticipate and address gaps in health service availability.
- chap9_li_2
7chap9_p_7Build credible execution capacity and data-driven delivery.
8chap9_p_8The instruments and mechanisms described herein rely on measurable results. If health-related indicators are perceived as weak or unreliable, debt management offices (DMOs) and PPP units will be reluctant to include them in new financing agreements. MoHs can strengthen their credibility by improving data systems, consistently tracking performance and publishing transparent results. Collaboration with technical and financial partners such as the Global Fund or Gavi can help demonstrate accountability and provide assurance to finance counterparts during negotiations. Similarly, MoHs need to build PPP project preparation capacity to prepare, appraise and monitor projects.
- chap9_li_3
9chap9_p_9Collaborate closely with the MoF to design and execute health financing instruments.
10chap9_p_10Health leaders should advocate for establishing regular coordination with the appropriate MoF departments. In working with the DMOs, PPP units or other responsible departments at the MoF, they can help identify indicators and project/programme pipelines that could underpin health-related finance instruments. Developing a joint communication and investor outreach strategy can be a concrete joint action by both ministries. By taking a proactive and propositional role, MoHs can help shape new instruments so that health priorities are integrated from the start and ensure that potential gaps can be addressed early on.
Recommendations for Ministries of Finance
- chap9_ol_1
- chap9_li_4
11chap9_p_11Put blended finance tools at the centre of national borrowing plans.
12chap9_p_12African governments have increasingly utilised blended finance to fund development projects, thereby lowering the cost of funding and ensuring market access. To maximise impact, the MoF could leverage health priorities established by the government to deepen and broaden credit enhancement opportunities beyond traditional guarantors and insurers, diversifying towards global health donors. Bespoke health-related structures that combine multiple credit-enhancement schemes could therefore be developed. Additionally, the MoH could identify PPP options that could benefit from specific debt instruments that increase fiscal space for long-term PPP commitments.
- chap9_li_5
13chap9_p_13Establish an interministerial sustainable finance committee.
14chap9_p_14Establishing a cross-government committee or task force will foster early collaboration among relevant line ministries directly involved in mobilising sustainable finance. This platform will help MoFs coordinate efforts across sectors, reduce bottlenecks and streamline the entire process of structuring and implementing sustainable finance initiatives. The committee will identify/oversee project identification (building on the budget tagging system), elaborate on government commitments if required in potential debt swaps, formulate any necessary key performance indicators (KPIs), collect data and prepare annual reports as required by financing agreements. In the case of PPPs, cross-governmental cooperation ensures alignment of policy objectives, accelerates approvals and harmonises technical standards. By creating structured mechanisms for information sharing, joint decision-making and coordinated oversight, governments can streamline project development, enhance risk allocation and provide more explicit guidance to private partners.
- chap9_li_6
15chap9_p_15Ensure visibility over budget execution for the health sector.
16chap9_p_16The MoF - or the ministry responsible for the budget, if relevant - should strengthen oversight of health sector expenditures at the national and subnational levels of government to ensure transparency and accountability. Regular monitoring and reporting of budget execution will identify discrepancies early on. Implementing integrated data systems with support from technical partners (e.g. the United Nations Development Programme (UNDP) and global health institutions) can enhance visibility and facilitate funds allocation reporting, where this is relevant. Clear dissemination of expenditure data will also build trust with stakeholders and development partners. Ultimately, this approach will optimise health funding use and support improved health outcomes.
- chap9_li_7
17chap9_p_17Strengthen Accountability and Reporting Capacity.
18chap9_p_18Given the legally binding nature of reporting obligations in financing contracts, MoFs should ensure the MoH has adequate capacity - internally or through technical assistance - to monitor compliance with KPIs and/or commitments required to be given in the context of the proposed transactions and report on funding allocation on a timely basis. This safeguards compliance and builds investor confidence. In the case of a PPP, the MoH and MoF should build capacity to monitor the PPP’s execution and ensure continued value for money, as well as substantial health impacts from the contract.
Recommendations for the International Finance Community
19chap9_p_19While national authorities (MoFs and MoHs in particular) have a primary role to play in identifying the health-financing gap and mobilising the relevant financing to fill it, international organisations (such as multilateral development banks (MDBs), DFIs, health-related institutions and private institutions) can play an enabling role.
20chap9_p_20The following recommendations aim to transform health-financing projects into realities and scale them up. African MoFs and MoHs should also seize the opportunity to advocate for the following recommendations to enhance sustainable financial flows and support improved health outcomes.
21chap9_p_21
- chap9_ol_2
- chap9_li_8
22chap9_p_22Standardise and improve health finance data.
23chap9_p_23Addressed to: International Capital Market Association (ICMA), Loan Market Association (LMA), the World Health Organisation (WHO), World Bank, other MDBs and regional development banks.
24chap9_p_24International standard setters (such as ICMA and LMA) and development partners should collaborate to standardise health-related debt instruments and enhance the quality of data underlying them. Strengthening the existing social sustainability-linked bond and loan principles with clearer, health-specific taxonomies of eligible expenditures and KPIs (aligned with both global health priorities and national health budget structures) would provide greater clarity and comparability across issuances. These efforts should be supported by the creation of an open-access platform that collects and updates health-related indicators for African countries, along with additional guidance on reporting and monitoring health impacts.
- chap9_li_9
25chap9_p_25Establish a task force to mobilise credit enhancement for health funding.
26chap9_p_26Addressed to: MDBs, DFIs, global health institutions (WHO, Gavi, Global Fund), donors.
27chap9_p_27Major credit enhancers should establish an action-oriented taskforce to coordinate and bolster credit enhancement for health funding. A structured dialogue among credit enhancers (ideally leveraging existing initiatives, such as the Task Force for Credit Enhancement for Sustainability-Linked Sovereign Financing), global health institutions and donors could explore a joint offering to governments and investors. The goal is to define a straightforward menu of credit enhancement options, reduce deal-by-deal uncertainty and build investor and issuer/borrower confidence in the viability of health swaps and sustainability-linked financing. Based on concrete cases and requests, the task force could seek to identify potential synergies among credit enhancers to co-guarantee debt instruments for healthcare. Given the lack of credit enhancement mobilisation in health, the task force could initially focus on initiating pilot transactions and drawing lessons from those experiences.
- chap9_li_10
29chap9_p_29Build the capacity of the MoF and the MoH to engage in innovative financing instruments jointly.
30chap9_p_30Addressed to: Capacity building institutions (e.g. African Development Bank (AfDB), African Legal Support Facility (ALSF), Macroeconomic and Financial Management Institute of Eastern and Southern Africa (MEFMI), West African Institute for Financial and Economic Management (WAIFEM), International Monetary Fund (IMF), World Bank).
Development partners should build capacities to bridge the technical gap between MoFs and MoHs. Regional and national training programmes targeting mid-level officials in debt management offices, budget directorates, PPP units and MoHs would help participants identify the right instruments for the right policies and initiate collaborations. This User Guide can serve as a core training material. These initiatives should also include in-country missions aimed at stimulating coordination between MoFs and MoHs. Over time, such programmes would strengthen technical understanding, promote joint ownership of financing solutions and foster national champions capable of driving technical efforts and political buy-in. Beyond training, institutions could help establish the necessary frameworks to facilitate a more substantial uptake of debt or PPP instruments.
28chap9_p_28
Glossary
1glossary_p_1Acceleration
2glossary_p_2a clause in a contract, typically a loan or a bond, allowing a creditor to request earlier repayment of the debt if a stated event occurs.
3glossary_p_3Agent
4glossary_p_4the financial institution acting as a representative of the lenders under a syndicated loan. The agent’s role is to administer the loan, make specified decisions on behalf of the lenders, provide the lenders with the necessary information for their decisions, and enforce the contract in the event of default.
5glossary_p_5Arranger
6glossary_p_6the financial institution engaged by a borrower to facilitate the issuance of a debt in the capital market.
7glossary_p_7Availability Indicators (AIs)
8glossary_p_8technical and operational measures that determine whether a health facility, or part of it, is available for use, which can affect availability-based payments under a PPP.
9glossary_p_9Availability Payment
10glossary_p_10a payment made by a procuring entity to a private partner in a PPP project based on the facility or service being available for use at the agreed performance standards.
11glossary_p_11Bilateral Debt Swap
12glossary_p_12a swap between two (sets of) parties, I.e. the debtor and the creditor (or a group of creditors).
13glossary_p_13Blended Finance
14glossary_p_14the strategic use of international financial institutions and multilateral development banks for the mobilisation of commercial finance towards sustainable development in developing countries.
15glossary_p_15Blue Bond
16glossary_p_16a debt instrument issued by a borrower to finance marine- and ocean-based projects with positive environmental, economic and climate benefits. The green bond concept inspires the blue bond.
17glossary_p_17Bond
18glossary_p_18a tradeable financial instrument representing a debt, issued by sovereigns, state-owned enterprises or corporates in the capital markets.
19glossary_p_19Call Option
20glossary_p_20an option to buy assets at an agreed price on or before a particular date, which can be included in the terms of a bond.
21glossary_p_21Civil Society Organisation (CSO)
22glossary_p_22a non-governmental, non-profit group operating outside of government control, formed by citizens to advance shared interests, provide services, or advocate for social, economic or political causes.
23glossary_p_23Climate Resilient Debt Clause (CRDC)
24glossary_p_24a contractual provision enabling the borrower to temporarily defer debt service payments (principal and/or interest) for a pre-agreed period when a predefined event occurs; also called a natural disaster or debt pause clause.
25glossary_p_25Collateral
26glossary_p_26an asset that a borrower offers as a way for a lender to secure the loan.
27glossary_p_27Commercial Debt Swap
28glossary_p_28is a transaction whereby private sector debt is replaced with a new instrument under more favourable terms (also referred to as a debt conversion).
29glossary_p_29Contingent Liability
30glossary_p_30a potential liability which becomes an actual liability upon the occurrence of an uncertain future event.
31glossary_p_31Contract Monitoring Regime
32glossary_p_32a structured system, processes and tools used by a procuring entity to track, verify and evaluate the private partner’s performance against the obligations set out in the PPP contract.
33glossary_p_33Country Coordinating Mechanisms (CCMs)
34glossary_p_34national multi-stakeholder bodies that coordinate, oversee and submit funding requests for global health programmes by bringing together government, civil society, affected communities, and development partners.
35glossary_p_35Coupon
36glossary_p_36the periodic payment as paid to the holder of a bond.
37glossary_p_37Credit Rating Agency (CRA)
38glossary_p_38an institution that provides investors with information and ratings about a borrower’s ability to meet its obligations.
39glossary_p_39Debt Conversion
40glossary_p_40is a transaction whereby private sector debt is replaced with a new instrument under more favourable terms (also referred to as a commercial debt swap).
41glossary_p_41Debt Restructuring
42glossary_p_42a process where the debtor negotiates with creditors to reduce the loan’s interest rate, extend its repayment term or reduce its balance to avoid default.
43glossary_p_43Debt Sustainability
44glossary_p_44the ability of a government to meet its debt obligations without requiring debt relief or accumulating arrears.
45glossary_p_45Debt Sustainability Analysis (DSA)
46glossary_p_46an assessment that evaluates a country’s ability to meet its current and future debt obligations without incurring repayment difficulties or requiring significant policy adjustments.
47glossary_p_47Debt Sustainability Framework (DSF)
48glossary_p_48a framework for analysing a country’s borrowing decisions and assessing debt sustainability under baseline and stress scenarios.
49glossary_p_49Debt Swap
50glossary_p_50a transaction in which a portion of a country’s existing debt can be acquired at a discount and swapped for SDG/ESG-related goals or investments.
51glossary_p_51Debt-to-GDP Ratio
52glossary_p_52the ratio of a country’s government debt to its GDP, used to assess its ability to repay debt.
53glossary_p_53Development Finance Institutions (DFI)
54glossary_p_54specialised institutions that raise funds to finance development projects or initiatives in developing countries.
55glossary_p_55Discounted
56glossary_p_56debt trading in the secondary market for less than its par value.
57glossary_p_57Eligible Projects
58glossary_p_58a list of projects to which the proceeds of use of proceeds bonds may be applied.
59glossary_p_59Emerging Markets and Developing Economies (EMDE)
60glossary_p_60term used in economics to describe a group of countries that are in a state of rapid growth but still have lower levels of economic development than advanced economies.
61glossary_p_61Environmental Social Governance (ESG)
62glossary_p_62the three central factors commonly used to evaluate the sustainability and ethical impact of an investment.
63glossary_p_63Eurobond
64glossary_p_64an international bond issuance denominated in a currency not native to the country where it is issued.
65glossary_p_65Event of Default
66glossary_p_66a condition defined in a loan or bond agreement that, if it occurs, gives the lender the right to demand immediate repayment.
67glossary_p_67Export Credit Agency (ECA)
68glossary_p_68an institution acting as an intermediary between governments and exporters to issue export financing in the form of credit, insurance or guarantees.
69glossary_p_69First-Loss Partial Guarantee
70glossary_p_70a credit enhancement mechanism under which a guarantor agrees to absorb initial losses on a financing up to a specified amount or percentage, reducing the risk exposure of other creditors.
71glossary_p_71Framework
72glossary_p_72a document drawn up by the issuer outlining the green and/or social characteristics of projects financed by bond proceeds.
73glossary_p_73Gross Domestic Product (GDP)
74glossary_p_74the estimated total value of all finished goods and services produced within a country’s borders in a specific period.
75glossary_p_75Global Health Institution (GHI)
76glossary_p_76an organisation that works across countries to improve health outcomes by providing funding, expertise, research or coordination on major global health challenges.
77glossary_p_77Green Bond
78glossary_p_78a bond whose proceeds are used exclusively for environmentally sustainable projects (also referred to as a climate bond).
79glossary_p_79Health Masterplan
80glossary_p_80a comprehensive, long-term strategic plan that outlines a country’s healthcare priorities, infrastructure needs, service delivery models and investment requirements.
81glossary_p_81International Capital Markets Association (ICMA)
82glossary_p_82a global trade association that promotes well-functioning and sustainable capital markets by developing standards, guidelines and best practices for market participants.
83glossary_p_83ICMA Principles
84glossary_p_84guidance published by ICMA on sustainable finance instruments, including GBP, SBP, SBG and SLBP.
85glossary_p_85Independent Verification Agent (IVA)
86glossary_p_86an external party appointed to objectively assess and verify whether a borrower or issuer has met the pre-defined environmental, social, or performance targets set under a sustainability-linked instrument or similar agreement.
87glossary_p_87Input-Based Spending (IBS)
88glossary_p_88funding that focuses on the resources used rather than the outputs or outcomes achieved.
89glossary_p_89Intermediary
90glossary_p_90the middle entity in a trilateral swap, often performed by an SPV.
91glossary_p_91Issuer
92glossary_p_92a legal entity such as a corporation, investment trust, government or agency that issues securities to finance operations.
93glossary_p_93Key Performance Indicator
94glossary_p_94a measure of financial or operational performance used for monitoring and review.
95glossary_p_95Liability Management
96glossary_p_96procedures and techniques used by bond issuers to buy back, exchange or alter the terms of bonds.
97glossary_p_97Loan Market Association (LMA)
98glossary_p_98a trade body for the European, Middle East and African syndicated loan market that enhances market efficiency by developing standard documentation and providing guidance on best practices.
99glossary_p_99Medium-Term Debt Strategy (MTDS)
100glossary_p_100a debt management strategy that guides a government’s borrowing decisions over the next three to five years, outlining the preferred composition of public debt that balances cost and risk in line with the country’s macroeconomic and financial objectives.
101glossary_p_101Monitoring Results and Verification (MRV)
102glossary_p_102a system that tracks the progress of key performance indicators throughout the life of a sustainable finance instrument.
103glossary_p_103Net Present Value (NPV)
104glossary_p_104the present value of a sum of money in contrast to its future value.
105glossary_p_105Official Development Assistance (ODA)
106glossary_p_106government aid promoting economic development and the welfare of developing countries.
107glossary_p_107Par Value
108glossary_p_108the face value of a bond repayable at maturity.
109glossary_p_109Paris Club
110glossary_p_110an informal group of creditors whose role is to find coordinated and sustainable solutions to the payment difficulties experienced by debtor countries.
111glossary_p_111Performance Indicators (PIs)
112glossary_p_112metrics used to evaluate the effectiveness of a health facility’s operations and clinical services (where provided), where failure to meet PIs may trigger contractual consequences for the private partner.
113glossary_p_113Premium
114glossary_p_114the excess value added to the price or cost of a financial asset.
115glossary_p_115Private Sector
116glossary_p_116the part of the economy run by individuals and companies for profit.
117glossary_p_117Private Sector Loans
118glossary_p_118loans granted by commercial banks or funds on specific terms.
119glossary_p_119Procuring Entity
120glossary_p_120a government ministry, state department, state-owned agency, municipal authority or other public authority responsible for planning, designing, tendering and managing a PPP project.
121glossary_p_121Public-Private Partnership (PPP)
122glossary_p_122a long-term arrangement where a private party delivers and finances public infrastructure or services.
123glossary_p_123Public Sector
124glossary_p_124the general government sector plus government-controlled entities engaged in commercial activities.
125glossary_p_125Public Sector Debt
126glossary_p_126the aggregate of central government and SOE debt.
127glossary_p_127Quality Indicators (QIs)
128glossary_p_128metrics used to assess the overall quality of services, infrastructure, equipment or operations delivered by a health facility.
129glossary_p_129Refinancing Risk
130glossary_p_130risk associated with an obligation that may not be refinanced or may be refinanced only at a higher cost.
131glossary_p_131Request for Proposal (RfP)
132glossary_p_132an invitation to submit a proposal for a project or mandate.
133glossary_p_133Return on Investment
134glossary_p_134a performance measure that evaluates an investment’s profitability by comparing net profit to cost.
135glossary_p_135Risk Allocation
136glossary_p_136a process of identifying the risks in a PPP project and assigning each risk to the party - public or private - that is best able to manage, mitigate or absorb it.
137glossary_p_137Second Party Opinion (SPO)
138glossary_p_138an independent assessment confirming a sustainable finance framework or instrument’s alignment with international standards such as ICMA and LMA Principles.
139glossary_p_139Secondary Market
140glossary_p_140a market for the resale of already issued debt securities.
141glossary_p_141Social Bond
142glossary_p_142a bond financing or refinancing of social projects that achieve positive social outcomes.
143glossary_p_143Social Bond Principles (SBPs)
144glossary_p_144ICMA’s Social Bond Principles provide guidelines on structuring, disclosure and reporting.
145glossary_p_145Social Loan Principles
146glossary_p_146LMA’s Social Loan Principles provide guidelines on structuring, disclosure and reporting.
147glossary_p_147Sovereign
148glossary_p_148a government guarantee of the obligations of a third party.
149glossary_p_149Special Purpose Vehicle (SPV)
150glossary_p_150a legal entity created for a specific purpose, often used as an intermediary in a trilateral swap.
151glossary_p_151State-owned Enterprise (SOE)
152glossary_p_152a legal entity wholly or partially owned by a government for commercial activities.
153glossary_p_153Sustainable Development Goals (SDGs)
154glossary_p_154a set of 17 interconnected global objectives adopted by the United Nations to guide countries toward ending poverty, protecting the planet and ensuring prosperity for all by 2030.
155glossary_p_155Sustainability-Linked Bond Principles (SLBP)
156glossary_p_156ICMA’s Sustainability-Linked Bond Principles provide guidelines on structuring, disclosure and reporting.
157glossary_p_157Sustainability-Linked Bond (SLB)
158glossary_p_158a bond whose characteristics vary depending on whether the issuer meets ESG/SDG objectives.
159glossary_p_159Sustainability-Linked Loan Principles (SLLP)
160glossary_p_160LMA’s Sustainability-Linked Loan Principles provide guidelines on structuring, disclosure and reporting.
161glossary_p_161Sustainability-Linked Financing
162glossary_p_162financial instruments, such as bonds or loans, where financial characteristics (e.g. interest rate or margin) vary depending on the issuer or borrower’s achievement of pre-defined environmental, social or governance (ESG) performance targets.
163glossary_p_163Sustainability Margin Adjustment
164glossary_p_164is a flexible interest rate feature in SLLs where the borrower’s loan interest rate (margin) goes up or down (a “ratchet”) based on achieving predefined ESG targets, known as Sustainability Performance Targets, linked to KPIs. Meeting targets earns a discount (lower rate), while missing them can trigger a premium (higher rate), incentivising companies to improve their sustainability performance financially.
165glossary_p_165Sustainability Performance Targets (SPT)
166glossary_p_166measurable improvements in KPIs for sustainability-linked instruments.
167glossary_p_167Syndicated Loan
168glossary_p_168a loan issued by a group of lenders with standard terms represented by an agent.
169glossary_p_169Tender Offer
170glossary_p_170a public offer to buy securities from holders at a specific price at a particular time.
171glossary_p_171Thematic Bond
172glossary_p_172a financial instrument allowing investors to finance specific themes such as climate, health or education.
173glossary_p_173The Nature Conservancy
174glossary_p_174a global environmental organisation managing debt-for-nature swaps since the 1980s.
175glossary_p_175Total Health Expenditure
176glossary_p_176the sum of public and private spending on health, including preventive and curative services, family planning and nutrition, but excluding water and sanitation.
177glossary_p_177Trilateral Swap
178glossary_p_178a structure where an intermediary buys outstanding debt at a discount with new insured or guaranteed debt issued at par.
179glossary_p_179Universal Health Coverage
180glossary_p_180a health system which aims to ensure equitable access, financial protection, and quality care for everyone, regardless of income, location, or social status.
181glossary_p_181Use of Proceeds (UoP) Debt Instrument
182glossary_p_182a debt obligation where proceeds are earmarked for a specific eligible use.
183glossary_p_183Value-Based Healthcare
184glossary_p_184an approach prioritising improved patient outcomes relative to resources spent.
185glossary_p_185Value for Money
186glossary_p_186achieving the best balance between cost, quality and risk over a project’s life cycle.
187glossary_p_187Viability Gap Funding
188glossary_p_188a public financial support mechanism providing a capital grant to make a socially beneficial but financially unviable project attractive to private investors.
Further Reading
Health and Financing
1reading_p_1Africa Centres for Disease Control and Prevention. 2025. Africa’s health financing in a new era. Available at: https://africacdc.org/news-item/africas-health-financing-in-a-new-era-april-2025/
2reading_p_2Institute for Health Metrics and Evaluation. n.d. Health financing. Available at: https://www.healthdata.org/research-analysis/health-financing
3reading_p_3FP Analytics. 2022. The compounding economic dividends of global health investment. Available at: https://fpanalytics.foreignpolicy.com/wp-content/uploads/sites/5/2022/09/Compounding-Economic-Dividends-of-Global-Health-Investment.pdf
4reading_p_4Organisation for Economic Co‑operation and Development (OECD). n.d. Official development assistance (ODA). Available at: https://www.oecd.org/en/topics/policy-issues/official-development-assistance-oda.html
5reading_p_5World Bank. 2014. Revised guidelines for public debt management (English). Available at: http://documents.worldbank.org/curated/en/539361468170971115
Sustainability-Linked Financing
6reading_p_6Emerging Markets Investors Alliance. 2025. Enhanced labeled bond principles. Available at: https://www.emia.org/f/enhanced-labeled-bond-principles
7reading_p_7International Capital Market Association. 2024. Social bond principles (SBP). Available at: https://www.icmagroup.org/sustainable-finance/the-principles-guidelines-and-handbooks/social-bond-principles-sbp/
8reading_p_8International Capital Market Association. 2024. Sustainability-linked bond principles (SLBP). Available at: https://www.icmagroup.org/sustainable-finance/the-principles-guidelines-and-handbooks/sustainability-linked-bond-principles-slbp/
9reading_p_9Loan Market Association. 2025. Guidance on Social Loan Principles. Available at: https://www.lma.eu.com/application/files/9717/4298/0850/Guidance_on_Social_Loan_Principles_-_26_March_2025.pdf
10reading_p_10Loan Market Association. 2025. Guidance on Sustainability-Linked Loan Principles. Available at: https://www.lma.eu.com/application/files/3517/4298/0872/Guidance_on_Sustainability-Linked_Loan_Principles_-_26_March_2025.pdf
11reading_p_11Loan Market Association. 2025. Social loan principles. Available at: https://www.lma.eu.com/application/files/1317/4307/3886/Social_Loan_Principles_-_26_March_2025.pdf
12reading_p_12Loan Market Association. 2025. Sustainability-linked loan principles. Available at: https://www.lma.eu.com/application/files/2317/4481/8026/Sustainability-Linked_Loan_Principles_-_26_March_2025_.pdf
13reading_p_13Organisation for Economic Co-operation and Development. 2024. Sustainability-Linked Bonds. How to make them work in developing countries and how donors can help. Available at: https://www.oecd.org/en/publications/how-to-make-them-work-in-developing-countries-and-how-donors-can-help_7ca58c00-en.html
14reading_p_14Sustainable Sovereign Debt Hub. 2023. More for Less, Scaling sustainability sovereign debt. Available at: https://www.ssdh.net/resources/more-for-less
15reading_p_15World Bank. n.d. FAB: Finance, applied tools and benchmarking. Available at: https://esgdata.worldbank.org/tools/fab
Debt Swaps
16reading_p_16Finance for Development Lab. 2025. Allocation of Debt Swap Resources: Guiding Principles. Available at: https://findevlab.org/allocation-of-debt-swap-resources-guiding-principles/
17reading_p_17Finance for Development Lab. 2025. Can Debt-for-Development Swaps Become an Asset Class? Available at: https://findevlab.org/can-debt-for-development-swaps-become-an-asset-class/
18reading_p_18Finance for Development Lab. 2024. Debt-to-Sustainability Swaps (D2S): A Practical Framework. Available at: https://findevlab.org/debt-to-sustainability-swaps-d2s-a-practical-framework/
19reading_p_19G20 Joint Finance-Health Task Force. 2024. A Retrospective Analysis of Debt-for-Health Swaps. Available at: https://www.gov.br/g20/pt-br/trilhas/trilha-de-financas/financas-saude/2-a-retrospective-analysis-of-debt-for-health-swaps-a-report-commissioned-by-the-rockefeller-foundation-for-the-g20-jfhtf.pdf/@@download/file
20reading_p_20Green Climate Fund. 2024. Debt for climate swaps: exploring avenues and opportunities. Available at: https://www.greenclimate.fund/document/debt-climate-swaps-exploring-avenues-and-opportunities
21reading_p_21Hu, Y., Wang, Z., Zhou, S., Yang, J., Chen, Y., Wang, Y. & Xu, M. 2024. Redefining Debt-to-Health, a triple-win health financing instrument in global health. Globalization and Health, 20, Article 39. Available at: https://globalizationandhealth.biomedcentral.com/articles/10.1186/s12992-024-01043-x
22reading_p_22MIGA. 2025. Côte d’Ivoire Debt-for-Development Swap. Available at: https://www.miga.org/sites/default/files/2025-02/C%C3%B4te%20d%27Ivoire%20Debt-for-Development%20Swap.pdf
23reading_p_23The Global Fund. 2024. Debt2Health Overview. Available at: https://www.theglobalfund.org/media/3k1gvfom/publication_debt2health_overview_en.pdf
24reading_p_24The Nature Conservancy. 2023. Nature Bonds Project Toolkit (Version 1). Available at: https://www.nature.org/content/dam/tnc/nature/en/documents/nature-bonds-toolkit-v1-english.pdf
25reading_p_25The Nature Conservancy. 2023. New Debt Coalition for Climate and Conservation. Available at: https://www.nature.org/en-us/newsroom/new-debt-coalition-for-climate-and-conservation/
26reading_p_26World Bank. 2024. BOSIB Report. Available at: https://documents.worldbank.org/en/publication/documents-reports/documentdetail/099080524122596875/BOSIB170e4732504619bc417c0d0996ec21
Public-Private Partnerships
27reading_p_27African Development Bank. n.d. Public-Private Partnerships. Available at: https://www.afdb.org/en/topics-and-sectors/initiatives-and-partnerships/public-private-partnerships
28reading_p_28Asian Development Bank. 2008. Public-Private Partnerships. Available at: https://www.adb.org/sites/default/files/publication/29025/ppspb-public-private-partnerships.pdf
29reading_p_29Herzlinger, R.E., Moloney, E. & Beyersdorfer, D. 2014. La Ribera Health Department (A). Harvard Business School Case No. 315‑006. Boston, MA: Harvard Business School Publishing (Revised March 2021). Available at: https://www.hbs.edu/faculty/Pages/item.aspx?num=47807
30reading_p_30InsightSoftware. 2025. 25 Best Healthcare KPIs and Metric Examples. Available at: https://insightsoftware.com/blog/25-best-healthcare-kpis-and-metric-examples/
31reading_p_31Kamugumya, D. & Olivier, J. 2016. Health system’s barriers hindering implementation of public-private partnership at the district level: a case study of partnership for improved reproductive and child health services provision in Tanzania. BMC Health Services Research, 16, Article 596. Available at: https://bmchealthservres.biomedcentral.com/articles/10.1186/s12913-016-1831-6
32reading_p_32Le, S. M., Govindaraj, R. & Bredenkamp, C. 2020. Public‑Private Partnerships for Health in Vietnam: Issues and Options. International Development in Focus. Washington, DC: World Bank. Available at: https://openknowledge.worldbank.org/entities/publication/59663cf3-c893-51eb-8fe3-e9d8cd2e7c8c
33reading_p_33McGuire, C.M., Kaiser, J.L., Vian, T., Nkabane‑Nkholongo, E., Nash, T., Jack, B.W., & Scott, N.A. 2024. Learning from the end of the public‑private partnership for Lesotho’s National Referral Hospital network. Globalization and Health, 20, Article 1043. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC10921972/
34reading_p_34Njagi, E., Iloka, K., Wawira, S., Thiga, L. & Muraguri, N. 2025. Learning from the Kenyan experiment: Key takeaways for implementing managed equipment services in developing countries. Frontiers in Health Services, 5, Article 1361261. Available at: https://www.researchgate.net/publication/391237468_Learning_from_the_Kenyan_experiment_key_takeaways_for_implementing_managed_equipment_services_in_developing_countries
35reading_p_35Powles, J. & Hodson, H. 2017. Google DeepMind and healthcare in an age of algorithms. The Lancet, 390(10114), pp. 2816–2818. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC5741783/
36reading_p_36PPP Directorate Kenya. 2025. Kenya PPP Projects: Progress and Status Quarterly Report – September 2025. Available at: https://pppkenya.go.ke/ova_doc/kenya-ppp-projects-progress-and-status-quarterly-report-september-2025/
37reading_p_37PricewaterhouseCoopers. 2020. Value-Based Healthcare: Delivering Outcomes that Matter. Available at: https://www.pwc.com/m1/en/publications/documents/value-based-healthcare.pdf
38reading_p_38Tiik, M. & Ross, P. 2010. Patient opportunities in the Estonian Electronic Health Record System. Studies in Health Technology and Informatics, 156, pp. 171-177. Available at: https://www.researchgate.net/publication/44668701_Patient_opportunities_in_the_Estonian_Electronic_Health_Record_System
39reading_p_39World Bank. n.d. PPP in Health. Available at: https://ppp.worldbank.org/ppp-health
40reading_p_40World Bank. n.d. PPP Online Reference Guide: Introduction. Available at: https://ppp.worldbank.org/PPP_Online_Reference_Guide/Introduction
Credit enhancement
41reading_p_41Bloomberg. 2025. Walmart heir’s family office commits USD 100 million for debt swaps. Available at: https://www.bloomberg.com/news/articles/2025-11-06/walmart-heir-s-family-office-commits-100-million-for-debt-swaps
42reading_p_42DFC. 2024. World’s largest debt conversion for conservation of a river and its watershed completed in El Salvador. Available at: https://www.dfc.gov/media/press-releases/worlds-largest-debt-conversion-conservation-river-and-its-watershed-completed
43reading_p_43Sustainable Sovereign Debt Hub (SSDH). 2025. Scaling credit enhancement models for sustainability-linked sovereign financing. Available at: https://www.ssdh.net/resources/scaling-credit-enhancement-models-for-sustainabilitylinked-sovereign-financing
44reading_p_44Sustainable Sovereign Debt Hub. 2025. Task Force on Credit Enhancement for Sustainability‑Linked Sovereign Financing for Nature & Climate. Available at: https://creditenhancement.org/
Acronyms
1acronyms_p_1AfDB
2acronyms_p_2African Development Bank
3acronyms_p_3AI
4acronyms_p_4Availability Indicators
5acronyms_p_5AIDS
6acronyms_p_6Acquired Immunodeficiency Syndrome
7acronyms_p_7AIIB
8acronyms_p_8Asian Infrastructure Investment Bank
9acronyms_p_9ALSF
10acronyms_p_10African Legal Support Facility
11acronyms_p_11BFSF
12acronyms_p_12Belize Fund for a Sustainable Future
13acronyms_p_13BLT
14acronyms_p_14Build, Lease, Transfer
15acronyms_p_15BMZ
16acronyms_p_16German Federal Ministry for Economic Cooperation and Development
17acronyms_p_17BOO
18acronyms_p_18Build-Own-Operate
19acronyms_p_19BOOT
20acronyms_p_20Build-Own-Operate-Transfer
21acronyms_p_21BOT
22acronyms_p_22Build-Operate-Transfer
23acronyms_p_23BPAF
24acronyms_p_24Bahamas Protected Areas Fund
25acronyms_p_25CCM
26acronyms_p_26Country Coordinating Mechanism
27acronyms_p_27CD4
28acronyms_p_28Clusters of Differentiation 4
29acronyms_p_29CDC
30acronyms_p_30Centres for Disease Control
31acronyms_p_31COVID-19
32acronyms_p_32Coronavirus Disease 2019
33acronyms_p_33CRA
34acronyms_p_34Credit Rating Agency
35acronyms_p_35CSO
36acronyms_p_36Civil Society Organisation
37acronyms_p_37D2H
38acronyms_p_38Debt2Health
39acronyms_p_39DBFO
40acronyms_p_40Design-Build-Finance-Operate
41acronyms_p_41DFC
42acronyms_p_42Development Finance Corporation
43acronyms_p_43DFI
44acronyms_p_44Development Finance Institution
45acronyms_p_45DMO
46acronyms_p_46Debt Management Office
47acronyms_p_47DSA
48acronyms_p_48Debt Sustainability Analysis
49acronyms_p_49EHR
50acronyms_p_50Electronic Health Record
51acronyms_p_51EIB
52acronyms_p_52European Investment Bank
53acronyms_p_53EPC
54acronyms_p_54Engineering, Procurement and Construction
55acronyms_p_55ESG
56acronyms_p_56Environmental, Social and Governance
57acronyms_p_57FAB
58acronyms_p_58Feasibility and Ambitiousness
59acronyms_p_59FM
60acronyms_p_60Facility Management
61acronyms_p_61FP
62acronyms_p_62Family Planning
63acronyms_p_63GDP
64acronyms_p_64Gross Domestic Product
65acronyms_p_65GFF
66acronyms_p_66Global Financing Facility
67acronyms_p_67GHIs
68acronyms_p_68Global Health Institutions
69acronyms_p_69GLF
70acronyms_p_70Galápagos Life Fund
71acronyms_p_71GPRBA
72acronyms_p_72Global Partnership for Results-Based Approaches
73acronyms_p_73HCW
74acronyms_p_74Healthcare Worker
75acronyms_p_75HIPC
76acronyms_p_76Heavily Indebted Poor Country
77acronyms_p_77HIV
78acronyms_p_78Human Immunodeficiency Virus
79acronyms_p_79HRIS
80acronyms_p_80Human Resource Information System
81acronyms_p_81IBRD
82acronyms_p_82International Bank for Reconstruction and Development
83acronyms_p_83ICMA
84acronyms_p_84International Capital Market Association
85acronyms_p_85IDB
86acronyms_p_86Inter-American Development Bank
87acronyms_p_87IMF
88acronyms_p_88International Monetary Fund
89acronyms_p_89IT
90acronyms_p_90Information Technology
91acronyms_p_91IVA
92acronyms_p_92Independent Verification Agent
93acronyms_p_93KMC
94acronyms_p_94Kangaroo Mother Care
95acronyms_p_95KPI
96acronyms_p_96Key Performance Indicator
97acronyms_p_97KYC
98acronyms_p_98Know Your Customer
99acronyms_p_99LSTA
100acronyms_p_100Loan Syndications and Trading Association
101acronyms_p_101MDAs
102acronyms_p_102Ministries, Departments and Agencies
103acronyms_p_103MDB
104acronyms_p_104Multilateral Development Bank
105acronyms_p_105MEFMI
106acronyms_p_106Macroeconomic and Financial Management Institute of Eastern and Southern Africa
107acronyms_p_107MES
108acronyms_p_108Managed Equipment Service
109acronyms_p_109MIGA
110acronyms_p_110Multilateral Investment Guarantee Agency
111acronyms_p_111MoF
112acronyms_p_112Ministry of Finance
113acronyms_p_113MoH
114acronyms_p_114Ministry of Health
115acronyms_p_115MoInfra
116acronyms_p_116Ministry of Infrastructure
117acronyms_p_117MRV
118acronyms_p_118Monitoring Results and Verification
119acronyms_p_119MTDS
120acronyms_p_120Medium-Term Debt Strategy
121acronyms_p_121NDP
122acronyms_p_122National Development Plan
123acronyms_p_123NGO
124acronyms_p_124Non-Governmental Organisation
125acronyms_p_125nVCC
126acronyms_p_126New Velindre Cancer Centre
127acronyms_p_127OCT
128acronyms_p_128Optical Coherence Tomography
129acronyms_p_129ODA
130acronyms_p_130Official Development Assistance
131acronyms_p_131OECD
132acronyms_p_132Organisation for Economic Co-operation and Development
133acronyms_p_133OEM
134acronyms_p_134Original Equipment Manufacturer
135acronyms_p_135PCEF
136acronyms_p_136Private Credit Enhancement Facility
137acronyms_p_137PCG
138acronyms_p_138Partial Credit Guarantee
139acronyms_p_139PHIO
140acronyms_p_140Pandemic From Time to Time
141acronyms_p_141PIs
142acronyms_p_142Performance Indicators
143acronyms_p_143PPP
144acronyms_p_144Public-Private Partnership
145acronyms_p_145PRG
146acronyms_p_146Partial Risk Guarantee
147acronyms_p_147PRI
148acronyms_p_148Political Risk Insurance
149acronyms_p_149QIs
150acronyms_p_150Quality Indicators
151acronyms_p_151RfP
152acronyms_p_152Request for Proposal
153acronyms_p_153RfQ
154acronyms_p_154Request For Qualification
155acronyms_p_155RMNCAH-N
156acronyms_p_156Reproductive, Maternal, Newborn, Child, and Adolescent Health and Nutrition
157acronyms_p_157RSSH
158acronyms_p_158Resilient and Sustainable Systems for Health
159acronyms_p_159SBP
160acronyms_p_160Social Bond Principle
161acronyms_p_161SDG
162acronyms_p_162Sustainable Development Goal
163acronyms_p_163SLA
164acronyms_p_164Service Level Agreement
165acronyms_p_165SLB
166acronyms_p_166Sustainability-Linked Bond
167acronyms_p_167SLBPs
168acronyms_p_168Sustainability-Linked Bond Principles
169acronyms_p_169SLF
170acronyms_p_170Sustainability-Linked Financing
171acronyms_p_171SLLs
172acronyms_p_172Sustainability-Linked Loans
173acronyms_p_173SLLP
174acronyms_p_174Sustainability-Linked Loan Principles
175acronyms_p_175SPO
176acronyms_p_176Second-Party Opinion
177acronyms_p_177SPT
178acronyms_p_178Sustainability Performance Target
179acronyms_p_179SPV
180acronyms_p_180Special Purpose Vehicle
181acronyms_p_181TB
182acronyms_p_182Tuberculosis
183acronyms_p_183THE
184acronyms_p_184Total Health Expenditure
185acronyms_p_185UHC
186acronyms_p_186Universal Health Coverage
187acronyms_p_187U.K.
188acronyms_p_188United Kingdom
189acronyms_p_189UN
190acronyms_p_190United Nations
191acronyms_p_191UNDP
192acronyms_p_192United Nations Development Programme
193acronyms_p_193UNICEF
194acronyms_p_194United Nations Children’s Fund
195acronyms_p_195UoP
196acronyms_p_196Use Of Proceeds
197acronyms_p_197UQD
198acronyms_p_198Unfunded Quality Demand
199acronyms_p_199U.S.
200acronyms_p_200United States of America
201acronyms_p_201USD
202acronyms_p_202United States Dollar
203acronyms_p_203WACC
204acronyms_p_204Weighted Average Cost of Capital
205acronyms_p_205WHO
206acronyms_p_206World Health Organisation
Contact
1contact_p_1Contact informations will be visible here
Bibliographie
Ayres, 2020
Sara Ayres, « A Mirror for the Prince? Anne of Denmark in Hunting Costume with Her Dogs (1617) by Paul Van Somer », Journal of Historians of Netherlandish Art, vol. 12, no 2, Newark, été 2020, publication numérique.
Brejon de Lavergnée et Thiébaut, 1981
Arnauld Brejon de Lavergnée et Dominique Thiébaut, Catalogue sommaire illustré des peintures du musée du Louvre. II. Italie, Espagne, Allemagne, Grande-Bretagne et divers, Paris, éditions de la Réunion des musées nationaux, 1981.
Brownlee, 2014
Peter John Brownlee (dir.), Samuel F. B. Morse’s “Gallery of the Louvre” and the Art of Invention, Chicago, 2014.
Cantarel-Besson, 1992
Yveline Cantarel-Besson, Musée du Louvre, janvier 1797-juin 1798. Procès-verbaux du conseil d’administration du Musée central des arts, Paris, 1992.
Delieuvin et Franck, 2019
Vincent Delieuvin et Louis Franck (dir.), Léonard de Vinci, (catalogue d’exposition, Paris, musée du Louvre, 24 octobre 2019 – 24 février 2020), Paris, musée du Louvre Éditions et Hazan, 2019.
Dezallier d’Argenville, 1752
Antoine Nicolas Dezallier d’Argenville, Voyage pittoresque de Paris, ou indication de tout ce qu’il y a de plus beau dans cette grande ville en peinture, sculpture et architecture, Paris, 1752 (1re édition 1749).
Ducos, 2023
Blaise Ducos, Antoon Van Dyck. Catalogue raisonné des tableaux du musée du Louvre, Paris, musée du Louvre éditions, 2023, https://doi.org/10.57232/NNXJ7755, consulté le vendredi 1er août 2025. https://livres.louvre.fr/vandyck.
Eaker, 2022
Adam Eaker, Van Dyck and the Making of English Portraiture, New Haven et Londres, 2022.
Gautier, 1882
Théophile Gautier, Guide de l’amateur au musée du Louvre, suivi de la vie et les œuvres de quelques peintres, Paris, éd. G. Charpentier, 1882.
Habert et Scailliérez, 2007
Jean Habert et Cécile Scailliérez, « xvie siècle », in Élisabeth Foucart-Walter (dir.), Catalogue des peintures italiennes du musée du Louvre. Catalogue sommaire, musée du Louvre, département des Peintures, Paris, musée du Louvre Éditions et Gallimard, 2007.
Liedtke, 1989
Walter A. Liedtke, The Royal Horse and Rider, Painting, Sculpture and Horsemanship, 1500-1800, New York, 1989.
Millar, 1982
Oliver Millar (dir.), Van Dyck in England (catalogue d’exposition, Londres, National Portrait Gallery, 1982-1983), Londres, 1982.
Ribeiro, 2020
Aileen Ribeiro, « Boucher und die Mode » in Astrid Reuter (dir.), François Boucher. Künstler des Rokoko (catalogue d’exposition, Karlsruhe, Staatliche Kunsthalle, 14 novembre 2020 – 6 avril 2021), Cologne, Wienand, 2020.
Rumberg et Shawe-Taylor, 2018
Per Rumberg et Desmond Shawe-Taylor (dir.), Charles I. King and Collector (catalogue d’exposition, Londres, Royal Academy of Arts, 2018), Londres, 2018.
Salmon, 2018
Xavier Salmon, « Pastels du musée du Louvre. xviie-xviiie siècles », Paris, musée du Louvre éditions et Hazan, 2018.
Sainte-Beuve, s. d.
Charles Augustin Sainte-Beuve, « Mme de Pompadour », Causeries du lundi, Paris, Garnier frères, s. d. (5e éd.), tome deuxième.
Smith, 1829-1842
John Smith, A Catalogue Raisonné of the Works of the Most Eminent Dutch, Flemish and French Painters…, Londres, 1829-1842, 9 vol. dont un supplément.
White, 2021
Christopher White, Anthony Van Dyck and the Art of Portraiture, Londres, 2021.